Author: Joel Schofer, MD, MBA, CPE
Finance Friday Articles
Here are this week’s articles:
11 Personal Finance YouTube Channels You Should Be Watching
A Recession Is Coming (Eventually). Here’s Where You’ll See It First.
Borrow 30-Year and Invest The Difference?
Burnout Isn’t Always Caused by Work
Disability Insurance Works If You Can’t
Do You Need Bonds In Your Investment Portfolio?
How to Profit from Investing in 18-Hour Cities
How to Tell a Good Financial Advisor From the Rest
Medical student-loan financing: What to know before you sign
Stupid Doctor Tricks — Physicians’ Biggest Financial Mistakes
The Impact of Interest Rates & Inflation on Stock Market Valuations
Think Bigger – Financial Planning is Not Just Investing
This is What Happens as Societies Become Wealthier
TL;DR: The Best Finance Books in One Sentence
You Are the Average of the Five Physicians You Spend the Most Time With
Internal Medicine Specialty Leader Call for Applicants – O5/O6
BUMED is pleased to announce a call for applicants for the Internal Medicine Specialty Leader position. Interested candidates should submit a Letter of Intent, CV, Bio, OSR/PSR, last 3 FITREPs, and Command Letter of Endorsement to CDR Melissa Austin (e-mail address in the global) NLT 15 Sep 2019.
Throwback Thursday Classic Post – The Top 5 Critical FITREP Mistakes
(You can find all of my FITREP education here, including the FITREP Prep document.)
When I was a Detailer, I would review a lot of records for people who failed to promote. Over and over again I would see FITREPs that reflected poorly on the officer. A lot of the time they didn’t realize it was even an issue, and sometimes they did it to themselves. Here are the top 5 FITREP mistakes you want to make sure you don’t make:
- Getting anything other than an early promote (EP) when you are getting a 1/1 FITREP, also known as an “air bubble.”
If you are the only officer in your competitive category (meaning that you aren’t competing against anyone on that FITREP), make sure you get an EP. Just like a single air bubble, you should “rise to the top” and get an EP. If you don’t get the air bubble and get a promotable (P) or must promote (MP), it reflects poorly on you unless it is CLEARLY EXPLAINED in the narrative why you are getting a P or MP. Here you can see an officer who got a 1/1 MP in his/her last FITREP and how it would be noted at a promotion board:

For example, if your reporting senior doesn’t give newly promoted officers an EP, your narrative should say something like, “Newly promoted officers do not receive EP rankings.” Sometimes this happens because your reporting senior is an officer from another service and he/she doesn’t understand the “Navy rules” for FITREPs. Sometimes it happens because either you or your reporting senior wants to give you a P or MP so you can “show progression” and get an EP. If you want to show progression, do it on the overall marks, not the final promotion recommendation. For example, give yourself a 4.0 EP, then a 4.17 EP, and finally a 4.33 EP. DO NOT give yourself a P or MP if you are getting a 1/1 FITREP.
- Both officers in a competitive group of 2 getting a MP FITREP.
If you are in a competitive group of 2, your reporting senior should give 1 of you an EP and the other a MP. If he/she gives you both a MP, it reflects poorly on both of you. Most often this will happen at an operational command and/or when there are 2 officers who are competing but are in the same promotion year group. Make sure your reporting senior doesn’t take the easy road and give you both a MP. One of you should get the EP, and the other can get a MP with a strong narrative explaining why.
- Declining from an EP to an MP without changing competitive groups (or “moving to the left”).
Most often I would see this when a resident who was in a large competitive group was given an EP FITREP. Then when they graduate from residency, their competitive group shrinks and they don’t get an EP but are left with an MP. Here’s what it looks like on when projected at the promotion board:

If I was you, I’d fight this like a dog. If they can’t keep you at an EP and you didn’t do anything wrong to deserve this, make sure the reason for your drop from an EP to a MP is clearly explained in the FITREP narrative.
If this happens to you because you are changing competitive groups, like when you get promoted or move from residency/fellowship to a staff physician at the same institution, it is not a black mark in any way and is expected.
- Not getting a 5.0 in Leadership.
If you are writing your own FITREP, you can’t give yourself a 5.0 in every category, but of all the categories Leadership is probably the most important one. Make sure you give yourself a 5.0 in Leadership because that is what the promotion board is looking to promote, future leaders. Having less than a 5.0 can send a bad message to the board.
Sometimes you have no control over this, and sometimes you may deserve less than a 5.0 in Leadership, but do your best to get a 5.0 there if at all possible.
- Giving yourself an overall trait average less than your reporting senior’s average.
Every reporting senior has an overall trait average for each rank that includes all of the FITREPs that they’ve done for that rank. You want to try and find out what it is.
While a reporting senior can look up their average on BOL, you can’t. You can, though, see it on your Performance Summary Record if you’ve received a FITREP from them at your current rank. Although it changes every time they do more FITREPs, their average the last time they did a round of FITREPs can be found on your PSR and is highlighted below by the red arrow with blue text (this reporting senior had ranked 6 LCDRs and had an average of 3.50 at that time) on one of the slides from my FITREP video podcast:

If you have never received a FITREP from your reporting senior at your current rank, maybe your one of your friends has. The other way to find out their average is to ask your chain-of-command. Someone, usually the command’s FITREP coordinator, will know their average for your rank.
It is probably obvious that once you find out their average, you’d like to make sure you are above it. Sometimes there is nothing you can do to be above it because you are getting a P and/or you deserve to be below it, but make sure you don’t rank yourself below it if given the chance to write your own FITREP.
In summary, those are the top 5 FITREP mistakes I often see. If you are interested in learning more, grab a copy of your FITREP and watch this video podcast. In 45 minutes you’ll know everything you need to know to write effective FITREPs.
RDML James Hancock is the New Medical Corps Chief
Last Saturday, RDML James Hancock assumed the position of Medical Corps Chief from RDML Paul Pearigen. For those of you who would like to learn about RDML Hancock’s background, here is his military bio:
Thanks to RDML Pearigen for his years of leadership in the position.
38th Commandant of the Marine Corps Planning Guidance
Anyone with anything to do with the United States Marine Corps should read the new Commandant’s planning guidance:
Reader Question/Poll – NOB Fitrep vs New Guy/Gal Promotable (P) Fitrep – Which is Better?
Reader Question
I’m a LCDR MC officer. I’m new at my command and was passed over during my in-zone promotion board for CDR. My command is considering a NOB fitrep vs. a Promotable (P) fitrep. Do you have a recommendation on which fitrep will be more helpful for my promotion board?
Reader Poll
My Answer
In my experience, most physicians seem to prefer the NOB. We’ll see what the poll above says, though.
Personally, I don’t think it really matters very much. At the promotion board, both are easily explained and a getting a P as the new officer is expected, so it wouldn’t be a negative.
I would say that if you get a P you have already started the march to an MP and then (hopefully) an EP. If you take the NOB, then your next fitrep could be seen as your “new guy/gal P.”
This last point is why I’d prefer the P if it was me, but I don’t feel that strongly about it.
Surgeon General Statement on Military MTF Transition
UNCLASSIFIED// ROUTINE R 051709Z AUG 19 FM CNO WASHINGTON DC TO NAVADMIN INFO CNO WASHINGTON DC BT UNCLAS NAVADMIN 180/19 PASS TO OFFICE CODES: FM CNO WASHINGTON DC//DNS// MSGID/GENADMIN/CNO WASHINGTON DC/DNS/AUG// SUBJ/ NAVY SURGEON GENERAL STATEMENT ON MILITARY MEDICAL TREATMENT FACILITIES TRANSITION// RMKS/1. This NAVADMIN provides Sailors and their families with information about the transition of Navy military medical treatment facilities (MTF) to the Defense Health Agency (DHA). The Department of Defense Military Health System (MHS) is undergoing a transition as administration and management of the Services' hospitals and clinics are transferred to DHA. This is occurring over several years with a goal envisioned by Congress that the MHS become a more standardized and a more integrated system of healthcare services. The Services have been working closely with DHA on the details and specifics of this transition. 2. This transition should be seamless to you. During this transition, you should see no immediate impact to access, healthcare services, or the things you and your families need. As this is a new role for DHA, the Services have continued, and will continue, to provide support and assistance to ensure our MTF's remain fully functional, and there is no immediate impact to care or services during transition until DHA is able to assume full administrative and management responsibility. Likewise, our Fleet and Fleet Marine Force Commanders should see no changes in Fleet or Fleet Marine Force support. Medical and medical support services required for operational support, all personnel who provide those services, and all uniformed personnel will remain within the Navy lifelines and under Navy control. 3. This transition is a multi-year effort, which started for the Navy in October 2018 when Naval Hospital Jacksonville transferred under DHA's administration and management. On 1 October 2019, more Navy MTFs in the U.S. will transition to the DHA. OCONUS MTFs, in a phased approach, will transition after all CONUS facilities, with the transfer of administration and management completed no later than 30 September 2021. 4. As we shift administration and management responsibilities of these MTFs to DHA, it will create opportunity for Navy Medicine to increase focus on operational support and keeping Service Members healthy and on the job. It will also enable us to enhance focus on unit support during sustained high tempo operations while creating opportunities for us to better prepare the medical force to deliver high combat survival and support in the future. We make a commitment to every Sailor, Marine, and their family that we will provide them the best care our nation can offer and do all in our power to return them home safely and alive. This transition will assist us in honoring that commitment. 5. For additional information, contact your local MTF or ask your care providers. More information on the overall initiative can be found at https://navymedicine.navylive.dodlive.mil/. 6. We at Navy Medicine will always honor the trust placed on us to provide the best care possible to those who defend our freedom and their families. Wherever a Sailor or Marine goes, Navy Medicine will always be there. My commitment is to keep you fully informed as this continues. Thank you so much for the trust and faith you place in Navy Medicine every day. 7. Released by Ms. Steffanie B. Easter, Director, Navy Staff.// BT #0001 NNNN UNCLASSIFIED//
New Process to Get Non-Specialty Specific Medical Corps Billets/Positions – Due 16 SEPT 2019
PERS has come up with a new process for Medical Corps Officers to apply for positions/billets that are not specific to any one specialty. Pay attention to this! These are the kind of senior leadership jobs that get you promoted.
The new process is described in this PDF:
MC Non-Specialty Specific Billets Booklet
These are the files that give details on the positions and the file you need to use to apply:
More Sailor-Friendly Options for PCS Moves
MILLINGTON, Tenn (NNS) — Navy Personnel Command (NPC) leaders announced today that they are expanding options and capabilities offered to further improve the Permanent Change of Station (PCS) move experience for Sailors and their families. This comes only a few weeks after the release of MyPCS Mobile and more capabilities are expected in the near future.
As part of the Navy’s ongoing pay and personnel transformation efforts, NAVADMIN 184/19 announces a new pilot program in which participating Sailors can use the Government Travel Charge Card (GTCC) for PCS move travel expenses. The initial pilot population includes Active Duty Sailors who are existing GTCC cardholders, executing CONUS-to-CONUS moves with less than 30 days of combined travel and Temporary Duty under Instruction, and who are single or traveling with accompanied dependents.
“We are providing Sailors with more choice and control during the PCS move process by providing them with the option to use their GTCC for PCS-related travel expenses,” said Rear Adm. Jeff Hughes, NPC commander.
“We want Sailors to have the funds necessary to support their move readily available either through use of a requested electronic funds transfer/direct deposit (EFT/DD) travel advance or by using the GTCC,” Hughes said, adding, “It’s their choice based on what works best for their particular situation.”
Participating Sailors may now choose to use either the GTCC or request an EFT/DD travel advance to support move related costs; however, both may not be used simultaneously.
Sailors who elect to participate in the pilot program may use the GTCC for temporary lodging at their old or new permanent duty station, fuel for privately owned vehicles (POVs) used as part of PCS travel, and for lodging and meals en route to their new duty station. Additionally, if the Sailor is entitled, the GTCC may be used for Dislocation Allowance (DLA) related expenses normally associated with the establishment of a new household.
This pilot period allows us time to evaluate the rollout through all phases of the PCS process, receive feedback from participating Sailors and commands, and fix any unknown issues prior to expansion to the widest possible population of Sailors in the near future.
Additionally, NAVADMIN 183/19 announces the release of Lean Orders and a PCS Entitlements Calculator. Lean orders is a streamlined, simplified, and plain language orders format, providing a Sailor and family everything they need to know to execute a move on a few screens on a mobile device. Lean Orders and the full text orders will both be available in MyPCS Mobile and on MyNavy Portal (MNP). A PCS Entitlements Calculator will also be available to provide Sailors a tool to easily determine their PCS travel entitlements. The intent is for a Sailor and their Command Pay and Personnel Administrator (CPPA) to use this tool during the initial PCS planning phase, which may influence what options the Sailor may pursue regarding advances or card use. It is also useful when a Sailor fills out their travel claim at their new permanent duty station to ensure the claim disbursement is the correct amount.
“Simplifying the PCS process for Sailors is a priority area of effort within the MyNavy HR Transformation effort,” said Ann Stewart, Director, NPC Pay and Personnel Management Department, adding, “All of these new services are a direct result of what we are hearing from Sailors and their families during numerous fleet engagements. We’re listening and rapidly improving processes and fielding capabilities to best resource our Sailors and reduce the administrative burden on them, so they can focus on readiness, lethality, and improving their life/work balance.”
It is vital that Sailors work with their CPPA and GTCC Agency Program Coordinator when pursuing available options for their PCS move planning and execution. The MyNavy Career Center (MNCC) Contact Center is also a 24/7 option and may be contacted via email: askmncc@navy.mil or by phone at (833) 330-MNCC (6622).
Get more information about the Navy from US Navy facebook or twitter.
For more news from Chief of Naval Personnel, visit www.navy.mil/local/cnp/.
FY20 LCDR Promotion Notes and Stats by Specialty
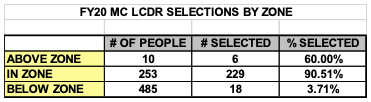
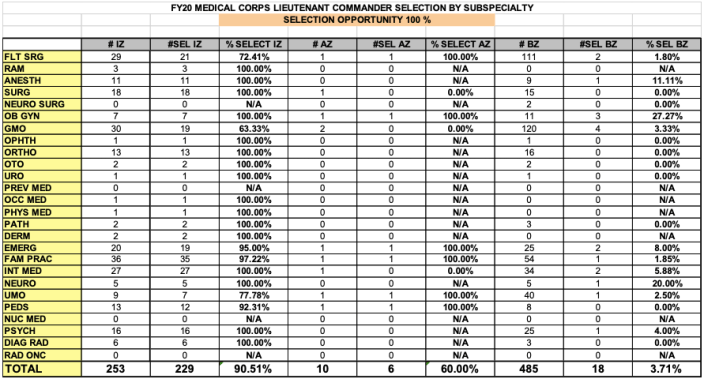
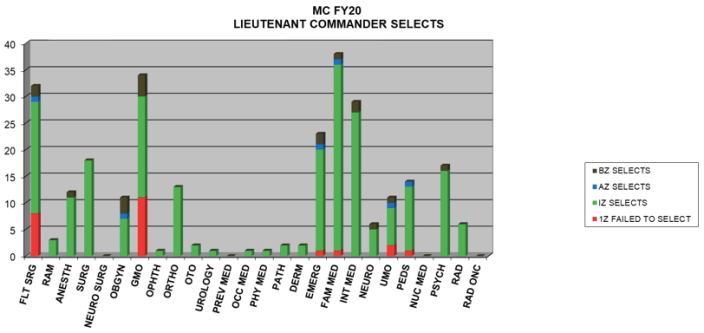
Here are the statistics for the recent LCDR promotion board and some notes from BUMED:
- 4 in zone individuals were auto-deferred due to having been on active duty less than a year.
- 90.5% of the in zone group were selected; the vast majority of those who were not selected had approved resignations.
- There were 6 above zone and 18 below zone selections. 7 of those 18 below zone selects were in General Medical Officer, Flight Surgery, or Undersea Medical Officer billets.