RDML James Hancock is the New Medical Corps Chief
Last Saturday, RDML James Hancock assumed the position of Medical Corps Chief from RDML Paul Pearigen. For those of you who would like to learn about RDML Hancock’s background, here is his military bio:
Thanks to RDML Pearigen for his years of leadership in the position.
38th Commandant of the Marine Corps Planning Guidance
Anyone with anything to do with the United States Marine Corps should read the new Commandant’s planning guidance:
Reader Question/Poll – NOB Fitrep vs New Guy/Gal Promotable (P) Fitrep – Which is Better?
Reader Question
I’m a LCDR MC officer. I’m new at my command and was passed over during my in-zone promotion board for CDR. My command is considering a NOB fitrep vs. a Promotable (P) fitrep. Do you have a recommendation on which fitrep will be more helpful for my promotion board?
Reader Poll
My Answer
In my experience, most physicians seem to prefer the NOB. We’ll see what the poll above says, though.
Personally, I don’t think it really matters very much. At the promotion board, both are easily explained and a getting a P as the new officer is expected, so it wouldn’t be a negative.
I would say that if you get a P you have already started the march to an MP and then (hopefully) an EP. If you take the NOB, then your next fitrep could be seen as your “new guy/gal P.”
This last point is why I’d prefer the P if it was me, but I don’t feel that strongly about it.
Surgeon General Statement on Military MTF Transition
UNCLASSIFIED// ROUTINE R 051709Z AUG 19 FM CNO WASHINGTON DC TO NAVADMIN INFO CNO WASHINGTON DC BT UNCLAS NAVADMIN 180/19 PASS TO OFFICE CODES: FM CNO WASHINGTON DC//DNS// MSGID/GENADMIN/CNO WASHINGTON DC/DNS/AUG// SUBJ/ NAVY SURGEON GENERAL STATEMENT ON MILITARY MEDICAL TREATMENT FACILITIES TRANSITION// RMKS/1. This NAVADMIN provides Sailors and their families with information about the transition of Navy military medical treatment facilities (MTF) to the Defense Health Agency (DHA). The Department of Defense Military Health System (MHS) is undergoing a transition as administration and management of the Services' hospitals and clinics are transferred to DHA. This is occurring over several years with a goal envisioned by Congress that the MHS become a more standardized and a more integrated system of healthcare services. The Services have been working closely with DHA on the details and specifics of this transition. 2. This transition should be seamless to you. During this transition, you should see no immediate impact to access, healthcare services, or the things you and your families need. As this is a new role for DHA, the Services have continued, and will continue, to provide support and assistance to ensure our MTF's remain fully functional, and there is no immediate impact to care or services during transition until DHA is able to assume full administrative and management responsibility. Likewise, our Fleet and Fleet Marine Force Commanders should see no changes in Fleet or Fleet Marine Force support. Medical and medical support services required for operational support, all personnel who provide those services, and all uniformed personnel will remain within the Navy lifelines and under Navy control. 3. This transition is a multi-year effort, which started for the Navy in October 2018 when Naval Hospital Jacksonville transferred under DHA's administration and management. On 1 October 2019, more Navy MTFs in the U.S. will transition to the DHA. OCONUS MTFs, in a phased approach, will transition after all CONUS facilities, with the transfer of administration and management completed no later than 30 September 2021. 4. As we shift administration and management responsibilities of these MTFs to DHA, it will create opportunity for Navy Medicine to increase focus on operational support and keeping Service Members healthy and on the job. It will also enable us to enhance focus on unit support during sustained high tempo operations while creating opportunities for us to better prepare the medical force to deliver high combat survival and support in the future. We make a commitment to every Sailor, Marine, and their family that we will provide them the best care our nation can offer and do all in our power to return them home safely and alive. This transition will assist us in honoring that commitment. 5. For additional information, contact your local MTF or ask your care providers. More information on the overall initiative can be found at https://navymedicine.navylive.dodlive.mil/. 6. We at Navy Medicine will always honor the trust placed on us to provide the best care possible to those who defend our freedom and their families. Wherever a Sailor or Marine goes, Navy Medicine will always be there. My commitment is to keep you fully informed as this continues. Thank you so much for the trust and faith you place in Navy Medicine every day. 7. Released by Ms. Steffanie B. Easter, Director, Navy Staff.// BT #0001 NNNN UNCLASSIFIED//
New Process to Get Non-Specialty Specific Medical Corps Billets/Positions – Due 16 SEPT 2019
PERS has come up with a new process for Medical Corps Officers to apply for positions/billets that are not specific to any one specialty. Pay attention to this! These are the kind of senior leadership jobs that get you promoted.
The new process is described in this PDF:
MC Non-Specialty Specific Billets Booklet
These are the files that give details on the positions and the file you need to use to apply:
More Sailor-Friendly Options for PCS Moves
MILLINGTON, Tenn (NNS) — Navy Personnel Command (NPC) leaders announced today that they are expanding options and capabilities offered to further improve the Permanent Change of Station (PCS) move experience for Sailors and their families. This comes only a few weeks after the release of MyPCS Mobile and more capabilities are expected in the near future.
As part of the Navy’s ongoing pay and personnel transformation efforts, NAVADMIN 184/19 announces a new pilot program in which participating Sailors can use the Government Travel Charge Card (GTCC) for PCS move travel expenses. The initial pilot population includes Active Duty Sailors who are existing GTCC cardholders, executing CONUS-to-CONUS moves with less than 30 days of combined travel and Temporary Duty under Instruction, and who are single or traveling with accompanied dependents.
“We are providing Sailors with more choice and control during the PCS move process by providing them with the option to use their GTCC for PCS-related travel expenses,” said Rear Adm. Jeff Hughes, NPC commander.
“We want Sailors to have the funds necessary to support their move readily available either through use of a requested electronic funds transfer/direct deposit (EFT/DD) travel advance or by using the GTCC,” Hughes said, adding, “It’s their choice based on what works best for their particular situation.”
Participating Sailors may now choose to use either the GTCC or request an EFT/DD travel advance to support move related costs; however, both may not be used simultaneously.
Sailors who elect to participate in the pilot program may use the GTCC for temporary lodging at their old or new permanent duty station, fuel for privately owned vehicles (POVs) used as part of PCS travel, and for lodging and meals en route to their new duty station. Additionally, if the Sailor is entitled, the GTCC may be used for Dislocation Allowance (DLA) related expenses normally associated with the establishment of a new household.
This pilot period allows us time to evaluate the rollout through all phases of the PCS process, receive feedback from participating Sailors and commands, and fix any unknown issues prior to expansion to the widest possible population of Sailors in the near future.
Additionally, NAVADMIN 183/19 announces the release of Lean Orders and a PCS Entitlements Calculator. Lean orders is a streamlined, simplified, and plain language orders format, providing a Sailor and family everything they need to know to execute a move on a few screens on a mobile device. Lean Orders and the full text orders will both be available in MyPCS Mobile and on MyNavy Portal (MNP). A PCS Entitlements Calculator will also be available to provide Sailors a tool to easily determine their PCS travel entitlements. The intent is for a Sailor and their Command Pay and Personnel Administrator (CPPA) to use this tool during the initial PCS planning phase, which may influence what options the Sailor may pursue regarding advances or card use. It is also useful when a Sailor fills out their travel claim at their new permanent duty station to ensure the claim disbursement is the correct amount.
“Simplifying the PCS process for Sailors is a priority area of effort within the MyNavy HR Transformation effort,” said Ann Stewart, Director, NPC Pay and Personnel Management Department, adding, “All of these new services are a direct result of what we are hearing from Sailors and their families during numerous fleet engagements. We’re listening and rapidly improving processes and fielding capabilities to best resource our Sailors and reduce the administrative burden on them, so they can focus on readiness, lethality, and improving their life/work balance.”
It is vital that Sailors work with their CPPA and GTCC Agency Program Coordinator when pursuing available options for their PCS move planning and execution. The MyNavy Career Center (MNCC) Contact Center is also a 24/7 option and may be contacted via email: askmncc@navy.mil or by phone at (833) 330-MNCC (6622).
Get more information about the Navy from US Navy facebook or twitter.
For more news from Chief of Naval Personnel, visit www.navy.mil/local/cnp/.
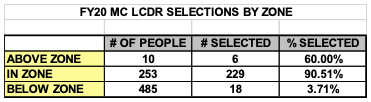
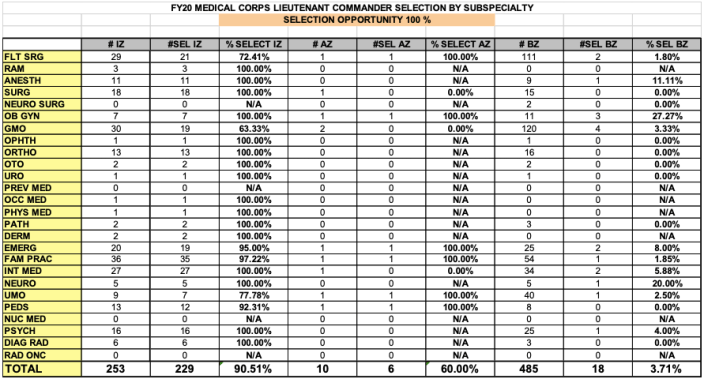
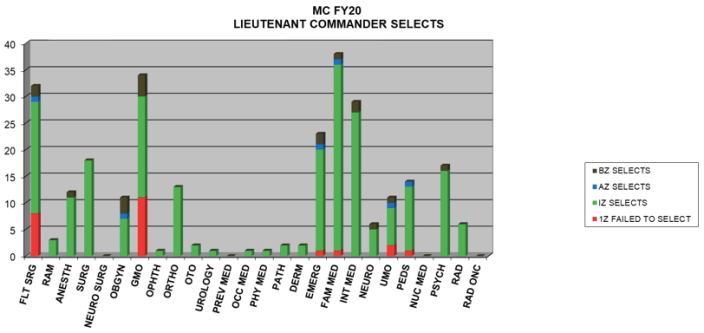
FY20 LCDR Promotion Notes and Stats by Specialty
Here are the statistics for the recent LCDR promotion board and some notes from BUMED:
- 4 in zone individuals were auto-deferred due to having been on active duty less than a year.
- 90.5% of the in zone group were selected; the vast majority of those who were not selected had approved resignations.
- There were 6 above zone and 18 below zone selections. 7 of those 18 below zone selects were in General Medical Officer, Flight Surgery, or Undersea Medical Officer billets.
How to Get Published in Medical School and Boost Your CV
Here’s a link to this article for all the medical students out there:
Finance Friday Posts
Here are this week’s articles:
5 Attributes That Make You An Easy Financial Target
5 Money Lessons from Adrian Peterson
Answering the top 5 questions about ETFs
Double Checking Your Investment Portfolio
Early Retirement Checklist Part Two: Insurance, Family, and Social Considerations Prior to FIRE
Financial Planning for a Special-Needs Child
FIology – Lessons in Financial Independence
Getting out of the Market in Retirement?
How Locum Tenens Saved My Life
How Much Time Does It Take To Manage My Own Properties?
In Praise of the Renaissance Man
Investing in a Negative Interest Rate World
Our Experience Buying a Brand New Car
Stop Tax Return Fraud: Sign Up For IRS IP PIN Program
The 5 Benefits of Financial Freedom
What Physicians Need to Know about Investing Before Hiring a Financial Advisor
Why Paying Down Debt Aggressively Was the Worst Financial Decision I’ve Ever Made
Throwback Thursday Classic Post – Moonlighting in the Navy
It’s August and a whole new crop of recent residency graduates can now moonlight for the first time in their Naval careers, so here is a video and blog post that discusses some of the basics of moonlighting.
Should You Moonlight?
I think the answer to this question depends on a lot of things. First, do you envision yourself working clinically when you leave the Navy? For most physicians, the answer to this question is yes, and depending on your specialty you may need to moonlight to maintain your clinical skills. We don’t always get exposed to the full scope of our specialty in the Navy. My wife is a pediatrician, and when she was on active duty I thought she had a full scope pediatric practice and did not need to moonlight to maintain her skills. As an emergency physician, though, it is rare to get exposed to the full breadth of emergency medicine in a Navy emergency department. You have to make an honest assessment of your specialty, the breadth of your Naval practice, and whether you need to moonlight to maintain your skills.
In addition, you need to figure out your motivation for moonlighting. A common motivation is to earn extra money, and that is a fine motivation, but you never want to make decisions that make you dependent on the money. You may deploy, your CO could take away your moonlighting privileges, or you could PCS somewhere where you can’t moonlight. You don’t want to be the bankrupt doctor because you bought a house you can’t afford without moonlighting.
The Navy’s Moonlighting Rules
In order to moonlight you have to get permission from your command. It is a privilege, not a right, and you can lose this privilege if you fail a PFA, don’t stay up-to-date on your training/readiness requirements, or don’t produce academically when required.
If you are going to moonlight somewhere outside of a 2 hour drive, you need to take leave. If you are flying anywhere, no matter the distance, you need to take leave. You can’t moonlight more than 16 hours/week and you need to have 6 hours of time off between clinical periods for your moonlighting job and your Naval duties. You’ll need to complete an annual attestation that says you are aware of these policies and compliant with them. If your specialty makes complying with these guidelines hard, you can ask for a waiver from your command.
Where Should You Moonlight?
If you moonlight locally you don’t need to take leave. If you can find a clinical setting you think you’d like after your time in the Navy is complete, you can even start working toward partnership.
If you work locum tenens, you can travel and sometimes chase “the big money.” If you work enough, the locum companies will cover all of your expenses, DEA, state licenses, travel, hotel, expenses, and malpractice insurance. Because you are likely traveling to a location more than a 2 hour drive away, you’ll need to take leave.
Basic Financial Planning for Moonlighters
Moonlighting allows you to put more money in tax advantaged retirement accounts. If you’re a non-moonlighter, you’d be limited to putting $19,000/year in the TSP and $6,000/year in your IRA (based on 2019 limits). If you moonlight and get paid on a 1099 as an independent contractor, you can fund a SEP IRA or solo 401k up to $56,000/year. It is rare that you’ll hit this maximum because you can’t moonlight enough to earn the amount required to do it, but you will be able to put more away than a non-moonlighter. A SEP IRA is easier to set up than a solo 401k, but a Solo 401k allows more money to be contributed at an equivalent salary. Plus, a SEP IRA messes up your backdoor Roth IRA contribution. For a great discussion on these two options, go to this article, but the bottom line is you’ll likely want to set up a Solo 401k and not use a SEP IRA:
http://whitecoatinvestor.com/sep-ira-vs-solo-401k/
Finally, moonlighters often want to incorporate because they think it provides malpractice protection, but that is a myth. Although there may be some tax advantages to incorporating, it doesn’t protect you from professional liability or malpractice.
Contract Pitfalls
If you are going to sign a contract, you are going to need to get some professional help. You should hire a healthcare or contract attorney to review any contract you are considering. You could also consider using a company that specializes in reviewing physician contracts like Contract Diagnostics. There are many issues you need to understand, including:
- Due process or termination clauses – For what reasons can they terminate you? Are you entitled to a hearing with the medical staff before your privileges are removed or restricted?
- Tail coverage – Does your malpractice insurance require tail coverage? If so, who is paying for it? Tail coverage is malpractice insurance that covers you after you stop working for that employer, and it can be VERY EXPENSIVE so you will want to know who is paying for it.
- TRICARE or VA eligible patients – You can’t bill these patients as they are already entitled to your services. This is spelled out very well in the moonlighting paperwork you will file with your command, but make sure your employer understands this.
Here are the Powerpoint slides for the video podcast below:
