FY-20 Active-Duty LCDR Staff Corps Promotion List
UNCLASSIFIED//
ROUTINE
R 071400Z AUG 19
FM SECNAV WASHINGTON DC
TO ALNAV
INFO SECNAV WASHINGTON DC
CNO WASHINGTON DC
CMC WASHINGTON DC
BT
UNCLAS
ALNAV 058/19
MSGID/GENADMIN/SECNAV WASHINGTON DC/-/AUG//
SUBJ/FY-20 ACTIVE-DUTY NAVY LIEUTENANT COMMANDER STAFF SELECTIONS//
REF/A/DOC/SECNAV/11JAN19//
AMPN/REF A IS THE FY-20 ACTIVE-DUTY NAVY LIEUTENANT COMMANDER STAFF PROMOTION
SELECTION BOARD CONVENING ORDER.//
RMKS/1. I am pleased to announce the following Staff Officers on the Active-
Duty List selected for permanent promotion to the grade of Lieutenant
Commander.
2. This message is not authority to deliver appointments. Authority to
effect promotion will normally be issued by future NAVADMINS requiring
NAVPERS 1421/7 preparation and forwarding of the document to PERS-806.
3. Frocking is not authorized for any officer listed below until specific
authorization is received per SECNAVINST 1420.2B.
4. For proper alphabetical order read from left to right on each line.
The numbers following each name to the right indicate the relative seniority
among selectees within each competitive category. Note: An (*) by the name
indicates the selectee was merit reordered to the top of the promotion list
in accordance with reference (a). Members are directed to verify their
select status via BUPERS Online.
Medical Corps
Algiers Timothy James 0129 Allan Elizabeth Jean 0135
Anderson Christine Lee 0127 Anderson Erik Lundberg 0054
Annis Heather 0040 Awodele Elizabeth Ann 0018
Baldeshwiler Mark J 0089 Banaag Shanley Hughes 0209
Barnett Patrick M 0137 Barrett Laura Danielle 0200
Beale Peter Alexander 0061 Beck Justin Lee 0210
Beckmann Robert C 0053 Beer Joshua Robert 0217
Berner Sara Beth 0012 Bessolo Andrew Michael 0132
Beyer Patrick Thomas 0172 Bianchi William David 0227
Biberston Jeffrey D 0138 Bond Emily Alison 0214
Booth Gregory James 0184 Bowen Michael Patrick 0058
Bradley Anthony S Jr 0023 Brawner Christopher M 0056
Brown Gary Orian 0192 Buel Katie Lauren 0190
Cannon Kathleen Ann 0083 Cayce Thomas Elliott 0049
Chauvin Meagan G 0201 Checchi Kyle Douglas 0047
Chece John Thomas 0006 Childers Benjamin Alan 0150
Clerc Jacqueline Gail 0078 Cole Jacob Henry 0252
Collins Jeannette R 0204 Cooper Ryan Thomas 0149
Cordes Mitchel F 0032 Costantoth Camille B 0097
Dear Thomas Augustus 0105 Decicco Joseph Daniel 0033
Desantis Kristin Marie 0126 Devore Charlotte E 0029
Deyoung Tracey H 0242 Dimond Leilani Lee 0088
Dombroski Eric Frank 0101 Donoughe John Scott 0008
Doudt Alexander Daniel 0087 Drayer Sara Marie 0240
Dugar Brandon Campbell 0072 Earley James Patrick 0151
Elliott Emily Jerniga 0243 Erdle Nicholas James 0106
Ernstsignore Elizabeth 0102 Eubanks Joshua David 0080
Ewing Christopher Kane 0017 Fang Ashley Lynn 0216
Fayos Zane Allyn 0142 Fehringer Adam Joseph 0236
Fenton Ronald C 0146 Fernicola Stephen D 0177
Fiore Benjamin Dylan 0130 Ford Alexandra Laine 0090
Fortner Grady A 0107 Freund Brin Etan 0016
Gambrell Justin Blake 0229 Garrett Andrew Robert 0235
Geddes Cody Michael 0231 Geurin Joel Preston 0206
Goold Michael Prince 0093 Gorman John Dunham 0232
Gosselin Michelle M 0024 Gosztyla Carolyn Emma 0114
Gould Allison Anne 0164 Grady Derek William 0144
Graf Andrew Clifford 0118 Granda Christopher S 0228
Gray Carrie Nicole 0073 Greenwald John Addison 0156
Griffis Clare Ellen 0128 Grim Andrew Ward 0079
Grounds Benjamin Eric 0179 Gurley Jessica Anne 0185
Gutierrez Lino A III 0022 Hamilton Ross Michael 0094
Harris Christopher W 0159 Harrison Kathryn Mary 0125
Hasson Ryan James 0136 Heig Todd W 0007
Held Jenny Michelle 0062 Heller Johnathan M 0034
Hendy Dylan Michael 0021 Hildreth Amy Follmer 0020
Hill Steven Michael 0085 Hill Susan Elena 0140
Hornacek Michael W 0123 House Tyler Bernard 0178
Houskamp Daniel John 0043 Hru Jessica Mahela 0113
Hughes Charlotte K 0121 Hughes Chase Andrew 0239
Hurdiss Sean Michael 0041 Hyman Leslie Jared 0213
James William F III 0038 James Kay Louise 0152
Johnson Andrew Steven 0050 Johnson Cody Reid 0202
Johnson William Rainey 0247 Jones Brendan Adam 0195
Jones Heather Louise 0092 Joseph Shane Paul 0133
Kim Cecilia Jung Ah 0175 Kitz Robert Joseph 0109
Kopp Jason Allen 0031 Kosmach Sterling N 0188
Kramer Todd Raymond 0193 Krepela Alyssa Leigh A 0173
Kucera Walter Bailey 0181 Kurth Benjamin James 0168
Landvater Jeremy Ray 0212 Lane Kelsey White 0064
Lavin Shane Thomas 0165 Lecourt Amarateedha P 0103
Lesko Joshua David 0246 Liddell Daniel Patrick 0244
Light Michael Lee II 0158 Lindsey Matthew C 0011
Litwin Aileen Joanna G 0067 Long James Owen 0111
Lovoi John Edward 0082 Lowery Matthew Joseph 0211
Mackey Meagan Orourke 0015 Madison Kristan E 0154
Maldonado Paul Anthony 0208 Manners Jody Lynne 0180
Marinides Zoe Olga 0183 Mcdevitt Joshua M 0234
Mcdowell Caroline M 0009 Mcevoy Christian S 0153
Mcguire Morgan Michael 0245 Mciver Ian James 0205
Mckinley Joseph Landon 0010 Mcneese Safiya D 0161
Mellor Thomas Edward 0169 Meyer Charles Deblois 0027
Mikals Kyle Arthur 0134 Ming Gerald 0124
Moon Patrick Sung Gook 0131 Morgan Lisa Lin 0241
Mullinix Patrick C 0057 Murnan Sean David 0248
Murphy Erin Alexis 0224 Myers Ryan Christopher 0037
Myers Shawn Michael 0221 Naymick Stephen A II 0207
Nguyen Alexandre D 0116 Nguyen Tuongvi Dang 0098
Nichols Christina E 0112 Noritake Alana Rae 0074
Norris Emily Ann 0060 Oliver David Scott 0249
Olsen Meredith Lutz 0187 Olsen Aaron Arthur 0197
Paloian Russell Joseph 0191 Park Jesse Aaron 0052
Paul Lauren Ashley 0220 Peacock Andrew Pringle 0115
Pelka Bryan Michael 0120 Perry Nicholas Peter J 0160
Pesqueira Jason M 0039 Peters John Daniel 0199
Petersen Kevin Thomas 0026 Pickett Maryanne Louis 0066
Pinches Helene Marie 0176 Plyler Sarah Elizabeth 0084
Porter Ian Michael 0048 Preston Ryan Kelburne 0095
Quacinella Michael A 0233 Rauschnot James C Jr 0225
Ray Mary Elizabeth 0059 Remick Stephen Robert 0025
Robinson Sara L 0155 Rose Thomas J 0100
Ross Heather Anne 0077 Rubado Eric Chad 0030
Salazar Alexander J 0071 Sanders Henry Sinclair 0003
Sanders Terrel 0065 Sarran Lauren C 0186
Schiavone Kaitlyn M 0219 Schwan Rory Daniel 0222
Schwer Ryan Peter 0145 Sears Stephen Carver 0108
Serpico Eric Joseph 0171 Shiv Erin Nichole 0163
Short Tyler Kent 0237 Sikes Michael Andrew 0035
Sing Derek Cheng Yung 0117 Slama Richard Eugene 0226
Smith Benjamin Thomas 0194 Spellman Kelli Rae 0070
Stark Michael David 0119 Stclair Jesse W IV 0198
Steele Clarence E 0143 Stefanowicz Jessica A 0189
Stockton Jon David 0046 Stottlemyre Morgan G 0148
Suggs Laura Caitlin 0215 Syski Andrew Lawrence 0081
Taillon Carolyn Edson 0157 Tam Tiffany Joy 0162
Teruya Kara Keiko 0086 Thomas Matthew Scott 0174
Tingzon Marlon Q 0230 Tompkins Brett Lowell 0091
Trainer Donald Ray 0036 Trentacosta Robert J 0253
Underbrink Troy P 0099 Verga Jared Michael 0218
Voss Ashley E 0196 Wackowski Gillian R 0223
Waggoner John Patrick 0005 Walker Karrie Anne B 0238
Wannemacher Nicholas Q 0096 Wasmund Joshua Brandon 0203
Weber Christopher Joel 0166 Weber Michael Conrad 0051
Weipert Michael James 0004 Weiss Merissa Ida A 0042
Weisse Angela Marie 0045 Wiemholt Edward B III 0141
Wiles Brittany Lynne 0182 Williams Barbara Jean 0122
Williams Jason Tyler 0028 Williamson Ryan Alan 0139
Wilson Davida E Y 0075 Wilson Benjamin Tsuba 0110
Wilson Matthew James 0063 Winslow Andrew Warren 0014
Wong Joshua Bryant 0055 Wray Jason Maurice II 0250
Wren Garrett Michael 0147 Wu Wei Wei 0069
Zah Angela 0251
Dental Corps
Aguigam Holly K 0050 Alexander Anthony S 0010
Baho Samantha Hee 0021 Baumann Kerry Beth 0013
Betterbed Thomas W 0052 Betz Sasha Jane 0003
Brown Lauren Ervin 0043 Buechele Ryan William 0035
Bussell Adam Peter 0023 Cardon Jonathan S 0056
Carter Megan Renee 0029 Christensen Jordan S 0054
Cole Diana Kay 0055 Collymore Page Linae 0017
Dachershapiro Judson A 0038 Daniel Catherine E C 0032
Daulton Ian Joseph 0057 Donaldson Blake Aaron 0033
Draper Eric Randall 0012 Dummett Scott Lee 0049
Eurick Kyle Andrew 0004 Evans Tracy Renee 0022
Ferretti Vincent J 0044 Fewins Jenna 0058
Freeark Jordan Thomas 0053 Harris Kristofer S 0001
Heeter Henry Benjamin 0027 Holliday John Lawrence 0026
Jenista John Steven 0037 Kantaris Kaely Marie 0047
Kelly Matthew John 0061 Kritzas Yianne George 0031
Lee Candace Joi 0051 Liu Wei 0040
Martin Ashley Ann 0016 Mckinney Richard Adam 0030
Mendoza Michael C 0045 Miller Justin Robert 0002
Moberg Jared Alan 0008 Mullen Bryan Robert 0028
Nguyen Thien Thong 0020 Norris Jessica Renee 0011
Novak Heidi Marie 0005 Owen Michael Richard 0039
Oxley Eric Blair 0060 Ragsdale Kyle William 0015
Randall Thomas Scott 0019 Readel Thomas John 0036
Rothwell David Joseph 0006 Sarmiento Kathrina M 0025
Sarwar Thamar Ansari 0007 Schmidt Carter James 0024
Simon Matthew Elliott 0042 Smith Stephen Estes 0018
Smith Whitney Aiko 0034 Spoelstra Michael P 0009
Takeda Ryan Toru 0048 Tangney Kyle Marshall 0059
Thompson Joseph R 0014 Uhrich Ross Martin 0041
Weinberg Allison Diane 0046
Medical Service Corps
Alba Alexander 0045 Alexander Emmy Jean 0070
Alleman Lee Armond 0110 Anderson Yekaterina L 0072
Armas George C 0100 Badic Janine Marie 0027
Bandermann Kyle M 0043 Beard Jason Bryan 0103
Bowerahming Michael L 0071 Boyer Robert Bain 0060
Brown Kevin Clayton 0091 Brown Nickita M A 0108
Bush Matthew Lane 0048 Camaya Victor M 0096
Caperton Ricky J Jr 0109 Castillo Christopher E 0039
Christy Nathaniel C 0112 Colton Matthew Aaron 0038
Cosgrove Sarah Emily 0086 Cutler Darren Wesley 0053
Do Nhu Quynh 0024 Druhl Carl Benjamin 0068
Ehrsam Mary Christine 0111 Evans Adrian Idris 0033
Fabunmi Bababowale O* 0004 Forrey Gabriel William 0035
Foss Pamela Cole 0101 Franks James Donald 0022
Garcia Daniel Cesar 0069 Garciarivera Jose A 0015
Gaxiola Laura Nicole 0105 Green Michelle Sereese 0080
Greenfield Richard T 0034 Gresko Derek Allen 0049
Grullon Emily Rose 0042 Haag Austin Jade 0006
Haden Brittany G 0094 Hallahan John P III 0051
Halwany Firdous D 0104 Harasimowitz Eric M 0054
Heath Christopher Jay 0041 Hebert Jeffrey Collin 0008
Hensley Philip D Jr 0106 Hermansen Brandon S 0093
Hoang Kevin Quoc Khoi 0050 Holifield Kenneth C 0066
Hsiang Jason Gordon 0074 Huang Ingrid Wilson 0012
Jairam Rohan Amir 0032 Jenkins Sarah Ann 0098
Johnson Margaret C 0056 Kenner Michael Ross 0059
Knight Rachel Ann 0009 Lacanilao Annaelisa P 0047
Lawler Tammi Lynn 0077 Leidel Jason Michael 0011
Lemma Jason Charles D 0090 Lenfert Amber Alayne 0058
Lester David Warren 0075 Logsdon Daniel Lyle 0065
Lugo Christopher 0102 Lund Daniel Paul 0088
Manasco Adrienne Joy 0014 Manning Michael Bryant 0019
Middleton Larry Jr* 0003 Montgomery Ralph R Jr 0113
Moore Joshua A 0097 Mowoe Austin Ochuko 0044
Muffett Joshua David 0099 Neuroth Michelle Renee 0087
Neville Andrew Michael 0081 Newman Safiat O 0023
Nobles Kelly Nicole 0028 Numanoi Mari Kino 0007
Nyberg Yuri Nicholaus 0026 Oconnor Kevin Matthew 0064
Orr Michael Dewayne 0084 Pascetta Joseph G 0040
Paturzzio Mindy Lee 0062 Pearson Mickenzie J* 0001
Peterson Ryan Lloyd 0031 Polito Michael A Jr 0052
Pollmanturner Courtney 0013 Porter Eric Andrew 0057
Quinn Roy Wayne 0079 Rabor Emiliano Calo 0076
Raza Saima Sadaf 0005 Reichold Adam Colter 0016
Riebel Laura Kathleen 0073 Robinson Nicola M A 0085
Romanperez Erick 0010 Saunders Jessica L 0078
Schermer Michael A 0030 Scott Chad Ryan* 0002
Selvarajah Kamalan 0018 Sharpe Linda Diane 0029
Shepard Kyle Hanson 0063 Shirley Ranjan A 0082
Siepker Alison 0083 Simmons Lamont Dewayne 0021
Simonds Wayne Glen 0046 Sterling William E 0092
Stopford Samantha Jane 0095 Sullivan John Lance 0036
Tailey Prince K 0020 Tan Paul Richard F 0025
Torrison Robert L 0107 Tran Hoang Harry Huy J 0061
Unruh Jason Cory 0037 Viano James Richard W 0055
Wearing Myra Samika 0089
Judge Advocate General's Corps
Baker Rachael E 0037 Bombard Robert Charles 0018
Breech Allyson Lee 0030 Bright Thomas John 0010
Bunkers Jessica House* 0001 Burkett Sarah Falvey 0016
Burman Damon Lamont 0036 Cardellino Matthew J 0013
Carroll Jennifer S 0024 Ceder Timothy C 0004
Corrigan Philip Joseph 0011 Elko Sharai Landesberg 0032
Fontenot Leah Michelle 0035 Foote Joshua D 0025
Hein Jonah A 0020 Holt Abigail Rose 0023
Horton Joseph Paul 0006 Howitt Caitlin Rachel 0033
Johnson Jennifer Lynn 0039 Juhn Jacqueline Misah 0022
Kissner Andrea May* 0003 Luzwick Allison June 0029
Marinos Megan Pauline 0028 Mccarl Lindsay Irene 0014
Mcmahon Catherine T 0007 Mcmahon Christopher C 0005
Portzer Joelle C 0026 Preis Ann Vodhanel 0034
Rausa Nicholas Joseph 0008 Sadhwani Alvir Ashok 0012
Santamaria Frank R 0027 Schwartau Jennifer H 0017
Scott Andrew Joyce 0031 Siladi Jonathan F 0038
Smith Adam Christopher 0009 Smith Karen Malia 0021
Solis Spenser Daniel 0040 Sonson Vincent Joseph 0019
Stamper Lucianna H* 0002 Wooten Sara Jane 0015
Nurse Corps
Aclese Ashley A 0070 Aranas Leonard N 0010
Argoncillo Kenneth B 0060 Barba Michelle 0066
Bartle Samantha L 0087 Beatty Stephanie Ann 0093
Bene Amy Lynn 0038 Boeder Katherine Mae 0018
Bonair Lauren E 0092 Braiotta Danielle M 0050
Caltagirone Megan Ann 0034 Carter James Nolan II 0057
Chiong Marie Frances N 0075 Clardy Katelin E 0067
Connell Christopher C 0020 Coronado Calina Marie 0021
Craft Ananda D 0097 Cross Mark Edward II 0030
Curry Candyce Marie 0102 Czarzasty Devon R 0052
Czubernat Lisa Suzanne 0026 Davis Shantel R 0023
Dougherty Shannon Lee 0071 Duarte Samira L 0037
Dunston Shaun David 0044 Ebili Patrick O 0008
Fears Burnetta F 0099 Fink Angelica Monique 0094
Fitzgerald Matthew D 0079 Foster Katelyn Ann 0078
Fowler Molly Eileen 0051 Frasure Sarah An 0059
Gallegos Tasha 0022 Gay Zebulon Daniel 0076
Giampaoli Agustin E 0054 Gibson Brandi Lynn 0025
Godfrey Chelsea R 0080 Gunter Larry Alton II 0061
Harper Kara Lynn 0007 Hays Kierstin Anne May 0040
Hendricks Michael Ryan 0082 Hennen Bryan Timothy 0077
Holmstrom Megan P 0017 Horigan Stephanie M 0058
Howell Jessica Rose 0095 Howell Krystal Mary 0064
Jackson Ruby Luz 0074 Jenkins Breda Helen* 0004
Kennovin Amanda Jill 0036 Kuelz Amanda Allison 0009
Kuhn Paul Eugene 0062 Latimer Emily Rose 0039
Lau Tiffany 0053 Lo Jennifer R 0063
Louk Sarah U 0046 Ludlow Clint Galen 0011
Mamaril Eugene E 0048 Mcgill Jesse Jordan* 0005
Mcginnis Tiffany C 0098 Miller Kathryn Ann 0072
Mix Lizetteanne C 0049 Morris Tameka Latoya 0033
Murphy Susan Ann 0029 Nguyen Billy Argus 0065
Njoroge Anthony N 0014 Oates Julianne Rose* 0003
Odriscoll Lisa Marie 0086 Ogungbe Olufemi O Jr 0083
Onwujiobi Samuel E 0085 Orozco Roberta Linda 0091
Parker Robin Lee 0027 Paul Uriah 0069
Payne Christopher G 0089 Quinn Brittany Hansen 0041
Reimonenq Ashley J 0047 Rios Rafael J 0028
Robinson Angela Sherie 0056 Rosales Angelica A 0068
Ryan Erin Rose 0100 Scott Kelly Ann* 0002
Sizemore Aileen David 0084 Smith Chad Everett* 0001
Stephan Lucy Padro 0043 Talvo Raben Bumatay* 0006
Thomas Stephanie D 0024 Tobias Kirra Kristen 0088
Tsuhako Brennda Ann 0073 Turner Constance Marie 0096
Vanhorn Shain Douglas 0055 Visser Lindsay Auman 0101
Voelkel Nathan Edward 0081 Wasson Aaron Nathaniel 0035
Wheelous Rachael Dee 0045 Whiteside Jade Tiari 0031
Whiteside Zachary K 0032 Williams Erin Mattie 0090
Wilson Samina 0042 Zelsdorf Gisselle I 0012
Supply Corps
Amposta Janpaul P 0029 Anderson Keith C 0052
Anschuetz Christopher 0068 Bellington Matthew S 0026
Bermudez Daniel C 0089 Bloxham Evan Raydel 0039
Brill Thad Robert Jr 0042 Brooks Mario Dion P 0091
Brown Christopher J 0087 Carney Tara Jill 0054
Castellanos Eduardo J 0032 Chu Calvin Thanh Hoang 0088
Colon Wanda Ivelize 0066 Crabb Jacob Colby 0024
Cruz Russell 0094 Cuff Stephen Alphonso 0084
Davis Dessislava I 0048 Davis Jacob Reed 0027
Deanon Aaron Benri H 0083 Deiter Jared Ray 0038
Delateur Emmett Louis 0046 Devlin Alanna Mary 0086
Diop Alioune S 0050 Disanto David Joseph* 0005
Dyal David A III* 0001 Ellis Kyle Paul 0071
Escobar Luis Carlos* 0008 Fuentes Madeleine 0030
Garrett Jami Michelle 0036 Gay Justin Chaz* 0002
Givens Jared Lyn 0080 Grayum Travis Michael* 0003
Grogan Shawn Michael* 0004 Guire Charles Walter 0011
Hague Arash 0055 Hamdouni Najib 0047
Harpel Aaron James 0023 Harpel Blake Michael 0074
Hatting Daniel Stewart 0035 Heisler Andrew Charles 0058
Hendricks Crette O II* 0007 Henry Ian Alexander 0044
Herrick Jonathan Andre 0056 Higgins Justin N 0028
Hinds Anthony Learie 0043 Hinkley Daniel F 0037
Hodsdon Bentley D 0015 Howell Brent James 0049
Hunnell Justin Michael 0059 Hutchings Amy Rose 0092
Irby Traci Leigh* 0006 Jacques Analee Huffman 0076
Jacques Peter Wesley 0078 Johnson Jonathan Leroy 0041
Jones Phillip Charles 0016 Ketring Jacquelyn Mei 0019
Kovachev Nicholas K 0022 Koye Stephen B 0057
Kung Michael Shihche 0013 Lamb Winston Callis 0064
Lopez John Froylan 0010 Machinporrata David R 0090
Martinez Anthony T 0018 Maryan Broward Clark 0093
Meyer Anthony Franklin 0073 Montgomery Jason Wayne 0009
Morlan Jason Ray 0085 Murphy Joseph Patrick 0067
Nechak Matthew Michael 0061 Okonak Jonathan M 0060
Ortiz Bryan Harmon 0077 Riverafontan Gamalier 0079
Roach Adam Michael 0025 Roberts Bret Masters 0082
Salami Saheed Abayomi 0020 Sceviour Gregory Paul 0070
Schoff Jeffrey Lynn 0021 Shane Patrick Charles 0033
Stephens Jordan Tyler 0072 Story Jason Leroy 0062
Suarez Pablo Harana 0063 Sullivan Christina Ann 0081
Thompson Tracy Marie 0012 Travis Jonathan R 0053
Vadala Timothy Patrick 0095 Villanueva Raymond 0031
Vu Tung Pham The 0075 Walsh Erin Cathleen 0034
White Orlando Jerrod 0014 Wiesman Michael Andrew 0045
Wilson Richard James 0069 Zamudio Michael Tyler 0065
Zheng Lin Lin 0040
Chaplain Corps
Amora Eduardo Beritos 0013 Bayer Adam Edward 0022
Carlson Kristian L 0020 Downey David Douglas 0019
Grady Christopher R 0008 Hart Jason Ryan 0021
Hickman Joshua Wade 0016 Jean Wilking* 0002
Johnson Klint Arley 0017 Kirschenbaum Brian J* 0001
Maloney Jonathon Ray 0014 Martin David Robert 0011
Murphy Mario Kenyon 0007 Owen Jason Douglas 0012
Peterson David Aaron* 0003 Porter Jason Thomas 0023
Rodgers Paul Benjamin 0006 Russell Keith Alan 0005
Shaw Jason J 0009 Tambur David Allen 0010
Warren Yonatan Moshe 0018 Williams Roilynn K 0015
Woodard Gregory Scot 0004
Civil Engineer Corps
Acosta Ramon 0021 Anderson Andrew B 0030
Berube Jonathan Paul 0033 Blauwiekel Joseph P 0029
Bly Joshua Patrick 0036 Castin Jonathan L 0023
Cotherman Andrew James 0014 Depersia Raul Roberto 0006
Durnan Patrick Emmett 0034 Eldred Daniel Robert 0031
Erwin Mark Russell 0025 Fletcher William T 0017
Greunke Justin T 0032 Hernandez Robert G 0013
Huber Elizabeth A* 0004 Huls Donald Allen 0007
Kaiser John Michael 0009 Kiel Jason Douglas 0015
Kim Jonathan J 0012 Korpi Andrew K 0024
Krushinski Kristen 0005 Laycock Ronald Barton* 0003
Mcguire Jonathan David* 0001 Mitsch Michael Gregory 0011
Painter Kevin T 0038 Palik Timothy Sean 0027
Payne Daniel Y 0026 Pouliot John Joseph 0020
Renoewick Celeste D 0010 Rovinsky Alexander Jr 0028
Sims Corinne Ann 0035 Stock Thomas Ryan* 0002
Trejo Vincent 0019 Uglow Ronald J 0018
Webb Samuel David 0008 Weber Morgan Charles 0022
White Casie Marie 0037 Yu Sen Feng 0016
Limited Duty Officer (Staff)
Catanese Matthew W 0003 Glover Grant Cassidy* 0001
5. Released by the Honorable Richard V. Spencer, Secretary of the Navy.//
BT
#0001
NNNN
UNCLASSIFIED//
Pentagon Finally Has an Assistant Secretary for Health Affairs
Here’s a link to this article from Military.com:
Pentagon Finally Has an Assistant Secretary for Health Affairs
August Edition of Health Affairs Focused on Military Health System
A special August edition of the journal Health Affairs, focused on military medicine and the MHS, is now available.
A listing of articles, with links to abstracts, is available at the journal’s table of contents:
https://www.healthaffairs.org/toc/hlthaff/38/8
Full articles are available to journal subscribers. An introductory article from editor of Health Affairs, available free to all readers, is below:
Date: Aug 5, 2019
Title: Military Health Systems
Source: Health Affairs
Author: Alan R. Weil
This month we examine the health systems that serve 1.4 million active duty
service members; provide care and coverage for another 8.1 million
reservists, retirees, and family members; and provide care for 9.0 million
veterans. As the Military Health System (MHS) goes through a major
restructuring, it also faces pressures and opportunities similar to those in
the civilian sector.
OVERVIEW
Terri Tanielian and Carrie Farmer describe the evolution of coverage for
military service members and their families from the 1880s to the current
TRICARE program. They note that almost 60 percent of those covered by
TRICARE are retirees or their dependents. The authors describe how TRICARE’s
evolution has mirrored that of private insurance, with the growth of managed
care, the adoption of patient-centered medical homes, and the recent
introduction of patient cost sharing.
Terry Adirim discusses the 2017 National Defense Authorization Act
requirement to consolidate the direct care system of “fifty-one inpatient
hospitals and medical centers and 672 ambulatory care, occupational health,
and dental clinics,” currently operated separately by the Army, Navy, and
Air Force, under a single authority. The hope is that a consolidated system
“can more effectively standardize care across the enterprise through the
implementation of standard clinical pathways, standard administrative
policies and procedures, and efficiencies realized by eliminating
redundancies in headquarters personnel and operations.”
An essential component of the MHS is its ability to deploy medical personnel
on a moment’s notice to remote, often austere settings. Paul Hutter and
coauthors describe the challenge of gaining and maintaining the skills
necessary to treat battlefield wounds when most training and medical
practice occurs in traditional clinical settings where patients with fairly
routine conditions are treated. The authors note that the current
consolidation of the MHS’s direct care system creates both opportunities and
challenges for achieving the goal of having a “ready medical force.”
QUALITY
In the United States there are significant racial disparities in the
prevalence of heart disease and the quality of coronary care. Muhammad
Chaudhary and coauthors analyze data from TRICARE and find “no difference in
[National Quality Forum]-endorsed quality-of-care metrics between African
American and white patients receiving coronary artery bypass grafting.” The
authors conclude that universal insurance and equal access can contribute to
reducing racial disparities in surgical care.
Peter Learn and coauthors describe the MHS’s participation in the American
College of Surgeons’ National Surgical Quality Improvement Program.
One-third of military hospitals participated in 2014, with all forty-six
qualifying hospitals participating in 2018. The authors find encouraging
trends of quality improvement in the earlier-adopting hospitals, adding to
the evidence that quality improvement collaboratives can have their desired
effect.
Craig Holden and coauthors examine unplanned readmission rates in military
health facilities. They find a significant reduction in seven-day
readmission rates for medical and surgical services in fiscal years 2011-18
, consistent with broad efforts in the health care system to reduce
readmissions.
CHILDREN
Children of parents who are injured while serving in the military are at
increased risk of various poor health outcomes. Elizabeth Hisle-Gorman and
coauthors examine data for children two years before and two years after
parental injuries and find that these children “received decreased
preventive health care and had increased health care visits for injury,
maltreatment, and mental health care and increased days on psychiatric
medications.” The authors also note “the lack of post-injury change in
visits for maltreatment, injury, and mental health care for children of
parents who sustained their injuries on the battlefield.”
Almost two million children receive coverage through TRICARE. Joseph
Zickafoose and coauthors compare the comprehensiveness of this coverage to
that of Medicaid and Affordable Care Act Marketplace plans in five large
states. Notable limitations of TRICARE relative to Medicaid are in the areas
of well-child visits for children older than age six and developmental
screening. Marketplace plans cover a set of services similar to those
covered by TRICARE, but often with significantly higher cost sharing.
Roopa Seshadri and coauthors analyze access and quality for children covered
by TRICARE. Overall, children on TRICARE are more likely to have complex
medical or mental health needs than children covered by other public or
private insurance programs. Children on TRICARE with special needs could
obtain referrals, but the authors conclude that “our findings suggest that
TRICARE-insured families might not have reliable access to care when their
children have special health care needs or behavioral health needs.”
ACKNOWLEDGMENTS
Health Affairs thanks Gail Wilensky of Project HOPE for serving as issue
adviser. We also thank the Uniformed Services University of the Health
Sciences and the New York State Health Foundation for financial support of
the issue.
https://www.healthaffairs.org/doi/full/10.1377/hlthaff.2019.00879
Sacred Cows Die As Marine Commandant Changes Course On Amphibs
Here’s a link to this thought provoking article:
Sacred Cows Die As Marine Commandant Changes Course On Amphibs
MCCareer.org The Book – Undersea Medicine Chapter
Brian M. Keuski, MD
Ian F. Eisenhauer, MD
Note: The views expressed in this chapter are those of the author(s) and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, or the United States Government.
INTRODUCTION TO UNDERSEA MEDICAL OFFICER (UMO):
Undersea Medicine is a small community within Navy Medicine, which primarily performs special duty physicals for divers, submariners, special operators, and nuclear-trained personnel. The Undersea Medical Officer (UMO) community, and those specialized communities that utilize UMOs, are high-tempo, actively deploying units ranging from Naval Special Warfare (NSW) to submarine squadrons. The role of the UMO is a mix of the general operational medicine that is expected of all General Medical Officers tailored to the specific duty concerns germane to the communities served. UMOs receive specialized training in these two key areas to ensure that they can adequately screen service members for conditions that could jeopardize the mission or lead to harm in diving, submarine or radiation health environments.
Medical administration (medical readiness, waivers/disqualifications, and the Independent Duty Corpsman (IDC) Program) takes up the majority of your time working as a UMO. UMOs train IDCs to tackle the challenging role of independent practice in austere environments with abbreviated training. UMOs must screen service members for illness that could overwhelm an IDC’s ability, as well as prepare IDCs to take care of those illnesses that arise with minimal access to MEDEVAC or specialty care. The key to success for a UMO will hinge directly on their ability to train those Dive Medical Technicians (DMTs) and IDCs who will ultimately perform patient care in the field.
UMO STRUCTURE AND JOB OPPORTUNITIES:
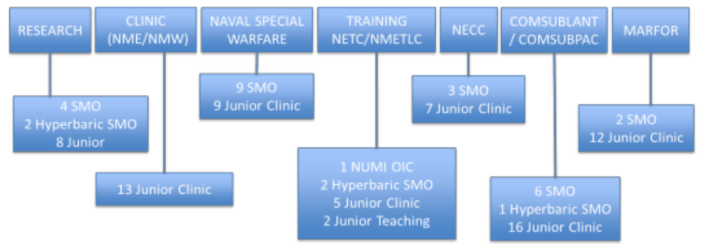
The UMO Community, as noted above, is a mix of submarine and diving support, organized by TYCOM-level leadership. UMOs fill billets assigned to the Marine Corps, Submarine Squadrons, Navy Special Warfare, Navy Expeditionary Combat Command (NECC), training commands, research commands, and Military Treatment Facilities as well as shipyard clinics. Most UMO roles are clinic-based. Completion of special duty physicals and leadership/mentorship of IDCs are the primary facets of the job. Some jobs incorporate diving into their role, while others have no associated diving. The many types of UMO billets are represented by categories, below.
The UMO Specialty Leader (M-95, Head Undersea Medicine) is located at the Bureau of Medicine and Surgery (BUMED) in Falls Church, Virginia, and oversees all of Radiation Health and Undersea Medicine. He/she makes recommendations to the waiver authority on all waivers and disqualifications of special duty standards. While all UMOs function under the oversight of the Specialty Leader, each has an operational chain of command. They either have a senior medical officer, or directly report as special staff to line officers in their daily duties. The above outline includes billets that are designated as senior officer billets, including some who are selected from the career milestone board, such as the Naval Undersea Medical Institute Officer-in-Charge (NUMI OIC) and Naval Submarine Medical Research Laboratory Commanding Officer and Executive Officer (NSMRL CO/XO), whereas others are open to any applicant. Second tour UMOs or senior UMOs will often have more opportunity to request billets, while those billets going to first tour UMOs will be chosen by the Detailer and Specialty Leader based upon their operational status, requirements, and “needs of the Navy.”
UMO APPLICATION:
UMO applications must be completed by the end of October, and selectees will be notified in December in parallel with graduate medical education (GME) selection. In order to prepare a successful application, UMO applicants must complete: a physical examination by a UMO (MANMED 15-102, 15-106), a passing Diver Candidate Physical Screening Test (PST) (MILPERSMAN 1220-410), two letters of recommendation, and a command letter of endorsement. A complete list of requirements can be found at the NUMI Website. Notably, these requirements represent minimum standards for training, but physical fitness well in excess of the minimums should be sought for a competitive application.
https://www.med.navy.mil/sites/nmotc/numi/UMOApply/Pages/default.aspx
Prospective UMOs historically have had the most difficulty with preparation for, and successful execution of the PST with a diver, as well as a letter of recommendation from qualified UMOs. The best resources for interns are nearby fleet UMOs or prior UMOs currently in GME training at your local MTF. These individuals can help you navigate the process, offer a recommendation letter, and administer your PST. If they can’t help you, the community is often small enough that they will know others that can. If no returning UMOs are within your intern class, ask upper level residents if they know any fleet returnees. Ultimately, the website above contains the contact information for the NUMI-POC, UMOC Mailbox, and the UMO Specialty Leader, each of whom will be willing to help you locate resources if you cannot otherwise. Letters of recommendation are also often difficult to complete. UMO letters of recommendation are designed to ensure you have considered why you are applying to the program, and to offer avenues for advice as you apply. If available during your intern program, scheduling an operational rotation with a local UMO can assist with the application requirements as well as show sustained interest.
The deadline for UMO application is in October; an interested applicant should complete the application in June-August to avoid an application being disqualified for missing requirements, including issues with medical standards that take time to process.
UMO PREPARATION:
Six months is a reasonable minimum amount of time to prepare for training prior to transferring to NUMI. Preparation must include learning multiple swim strokes, gaining in-water confidence, preparing to run significant distance, as well as improving callisthenic endurance. Below are outlined some minimum goals for reaching NUMI, though some factors that lead to success in school cannot be quantified. Ultimately, confidence in the water is the most important aspect of preparation for UMO training, and this takes time.
Be prepared to pass the PST with room to spare.
The Diver PST is a minimum standard that is used to ensure that candidates are ready to train. If you do not pass this ‘test’ on day one, you will be dismissed from training. Your swim will be in a cramped pool, with a shirt and UDTs on, and without goggles.
Some suggestions for success include:
- Train without goggles.
- Train in a crowded lane where you need to navigate around other swimmers.
- Swim with shorts and a baggy T-shirt to simulate the drag from the diver uniform.
- Become proficient, if not excellent, at sidestroke.
You also need to be prepared for the other events. Note that you will do your pull-ups after having just completed swimming, sit-ups, and push-ups. This fatigue causes issues for many people. Ten consecutive pull-ups prior to NUMI is a good minimum preparation for PST to compensate for this fatigue. If you currently can’t do any pull-ups, get multiple resistance bands, attach them to a pull-up bar (buy one and put it on your door – either at work or at home), and use as many bands as are necessary to be able to complete 6-8 pullups per set. When you can do 10 in a set, drop a band (or go to a smaller one). You should do pull-ups every other day, and you should do 50-60 at a minimum, which can be consecutive or broken up. If you do this for a few months, you will gain the required strength to do the pull-ups required for the PST.
Running is an important part of preparation for the PST. Being tired from upper body workouts and the aerobic stress of the pool will set you up to be slower than usual. You should be able to run your 1.5 miles in 11 minutes or under when you are fresh. Preparation can be with daily runs of 2-3 miles with 1 run per week designed to improve speed, and 1 run designed to improve distance. Examples of speed workouts may include Tabata runs or ¼ mile sprints, with a total distance of at least 1.5-2 miles (the length of the run portion of the PST) in sprints (e.g. 8 x ¼ mile sprints at goal pace, or under 1:50 per lap for an 11 minute time).
Be prepared to run for 5 miles at about an 8 minute mile pace.
While this may seem quick, you must recognize that you will be yelling cadences, running in formation, and carrying a guide-on flag. They will run you hard. Those who are unprepared for this type of distance often suffer stress injuries (shin splints, knee pain such as patellofemoral pain syndrome, etc.), so being prepared is crucial to making it through training. While at NUMI, they may not make you run this fast, but at NDSTC, some training teams will run significantly faster and farther.
Spend time doing hypoxia training (on land).
While breath-hold training in the water without supervision is dangerous, land-based training is very helpful in preparation for UMO training. There are many apps to teach you to hold your breath; STAmina Apnea Trainer, iHoldBreath, AIDA Freediving, and others. Having some comfort with a breath-hold allows a trainee to put their focus elsewhere during training. A 1:30 second breath-hold is a great starting place prior to starting at NUMI.
Get confident in the water.
You should be able to swim a minimum of 1000 meters in a workout, with mixed in push-ups, sit-ups, and pull-ups on the side of the pool. Calisthenic exercise mixed with swimming increases aerobic stress dramatically, and should be experienced before NUMI. Familiarity with breaststroke and freestyle are also useful, despite sidestroke and breaststroke being the only authorized swim strokes for the PST. Treading water is one of the most challenging factors of aquatic adaptability, and the eggbeater kick will make treading water easier. A trainee will need to be able to tread water with hands and elbows out of the water for a minimum of one minute. While methods other than eggbeater (frog kicks, flutter kicks, etc.) may seem easier at first, these methods break down when weight is held overhead. Becoming competent and confident while treading water will serve you well in training.
NUMI/NDSTC TRAINING PIPELINE, WHAT TO EXPECT:
The Naval Undersea Medicine Institute (NUMI) in Groton, CT is home to training for prospective Undersea Medical Officers. As noted above, preparation for this nearly six month training pipeline is crucial to success in becoming a UMO. The training pipeline is broken into three phases:
PHASE 1:
The First Phase of UMO Training is built around preparation for U.S. Navy Dive training at NDSTC. While there is a lot to learn to become an effective UMO, candidate failure is most often caused by quitting (drop on request -DOR) or an inability to meet the physical standards. Phase 1 physical preparation includes daily 1.5 hour workouts at 0500 to include running, calisthenics, swimming, in-water confidence training, practicing pool ‘hits,’ and other drills. The primary goals of UMOC preparation are PST preparation and in-water confidence training. This is where you will be introduced to over-unders, a repetitive under water swimming exercise. Preparation as noted above is highly encouraged to prepare you to start these exercises. While many UMOCs want to do over-unders prior to NUMI, the risk of shallow-water blackout is significant and has led to the death of skilled individuals. It is not recommended to do in water breath hold training before the safe training environment of NUMI. It is sufficient to become a great swimmer and have a good breath-hold prior to NUMI.
The time between workouts is spent learning radiation physics and health topics to complete the Radiation Health Indoctrination (RHI) certification. This certification prepares future UMOs to care for workers in the Radiation Health Program, as it allows UMOs to complete Radiation Medical Examinations (RMEs). This exam is required for Submarine personnel and Navy Divers who perform diving operations near submarines. The RHI Program also prepares UMOs to be the first line of defense in the event of a nuclear/radiologic casualty. Similarly, special duty physicals are introduced, an exam that certifies that specialized forces – including submariners, special warfare personnel, divers, radiation workers, and others – are able to complete their job effectively and safely without risking the safety of the mission or of the other crew.
UMOCs learn submarine medicine topics in phase I. In the submarine force, no person does a single job; it is the role of the entire crew to complete their main task, as well as to be prepared to address casualties, including fighting fires, addressing flooding, and even escaping the submarine. UMOCs complete training in these areas to understand ship systems and to be prepared to assist in these scenarios when/if they are aboard. UMOCs are also introduced to submarine culture and the hazards associated with submarine life.
PHASE 2:
The Second Phase of UMO training occurs on TAD orders to the Naval Diving and Salvage Training Center at the Center for Explosive Ordnance Disposal and Diving (CEODD). Prospective UMOs train like every other Navy Diver candidate with physical training both on land and in the water. Comfort in the water under extreme conditions is attained by breath-hold diving, treading with and without weights, surface swimming, teamwork drills, and many more activities. Training is built to ensure that candidates are sufficiently comfortable and calm in the water to train with equipment that can be dangerous if a diver were to panic. It should be noted that while traditionally this is where students fail out of the course, proper mental and physical preparation will prepare the vast majority of candidates.
The training includes qualification on the diving equipment used in the U.S. Navy. Competence with each piece of equipment is tested in both classroom and pool settings, to include SCUBA, KM-37 (Hard Hat Diving), and Mk-20 (full face-mask). There are also shorter familiarizations to re-breather equipment used by our forces. Most importantly for medical personnel, the course includes the Recognition and Treatment (R&T) of diving casualties course, which teaches candidates the medical knowledge required for treating diving related injuries. Topics span from basic dive physics to the latest theories on decompression sickness (aka ‘The Bends’), oxygen toxicity, and many other illnesses that can be seen in Navy Diving.
PHASE 3:
UMO training culminates in Groton, CT where comprehensive Oral Boards are performed for each candidate. Overseen by Naval Reactors, the nuclear power leadership of the U.S. Navy, this board includes questions about radiation health examinations, IDC oversight, special duty physicals, and diving related injuries. This phase also includes leadership education, operational medicine lectures, and helpful education in basic medical division officer roles and responsibilities. Most important to UMOs during this phase is assignment to a billet. While the process is variable, ranging from selection based upon course rank (merit-based) to direct assignment by the detailer, the process ultimately requires patience, as most UMOCs are post-intern physicians and have not yet experienced the flexible nature of Navy Orders. Once verbally assigned a billet, there are often multiple changes before final orders are cut. While this can lead to significant angst, it is important to recognize that this occurs all across the Navy. Remember, Navy orders can always be changed until the moment of execution!
JUNIOR UMO TOUR:
The junior UMO tour is variable based upon the billet location and type. While the specifics of each job will vary, there are a few aspects that are constant.
Junior UMO tour orders are for 2.5-3 years.
This means that for those UMO students in the summer class, you are able to complete your entire UMO requirement in 2.5 years and return to residency at that point. The winter class is only able to complete 2 years of their requirement, and if they wish to return at 3 years, must apply for a waiver of their commitment. Otherwise, they will spend 3 years at their job with a year of training (4 years total). While it is encouraged by BUMED and the Detailer to extend for the purposes of maintaining manning, some residencies are more receptive to extensions than others.
The Job of a junior UMO is to do Special Duty Physicals, supervise IDCs, and run medical programs.
There is a wide range among UMO billets in the number of patients, sick call visits, and special duty physicals daily. Being proficient at special duty physicals is what Navy Medicine expects, and will be a significant part of your job as a junior UMO. Similarly, overseeing the IDC program takes up a large proportion of a UMO’s time because of the role IDCs play in patient care. You must train them to be as independent as possible, because they work under your license with little oversight on a submarine or during austere operations.
Decide how operational you wish to be.
In general, clinic, submarine, and education jobs do not deploy, while Navy Expeditionary Combat Command (NECC), NSW, and Marine Diving billets will deploy. If you wish to do so, however, there are opportunities to be more operational from any billet. The unique training section below covers some opportunities to be operational/underway, and can be a good way to supplement a more clinic-oriented position. Getting involved with the local dive locker can also be a way to supplement a clinic-based role.
SUBMARINE WARFARE QUALIFICATION:
The Submarine Warfare Qualification is the main Additional Qualification Designator (AQD), and the only warfare qualification available solely to UMOs. Completion of a three-part process is required to achieve the Submarine Medical Officer (SMO) qualification. This process is overseen by NUMI instruction 5420.2 (series). Each applicant must complete the SMO Qualification Examination with an 80% or better. It can be requested from the current NUMI Instructor (UMO) at any time during the tour. They must also complete 30 days underway, or 15 days for those at commands without submarine responsibilities. This underway time includes completion of a SMO qualification card, including a formal board while underway. This time can be challenging to complete for some billets, and waivers will be considered for specific reasons outlined in the instruction above.
Finally, a technical paper or thesis is required to complete the SMO qualification. This process can be more challenging and should be started as early as is possible. The topic must be related to submarine medicine, diving medicine, special operations medicine, or radiation health. Once a topic is devised, approval for the topic should be sought by submitting a brief proposal with a comprehensive bibliography. The ultimate thesis format and substance is explained within NUMIINST 5420.2, however it can be summarized as similar to a scientific paper in length, content, and requirements. Once all of these requirements are met, a final application for recognition of your warfare qualification completes the process.
RETURNING TO RESIDENCY:
There are two schools of thought during the UMO tour. One mindset to have is to read voraciously, seen patients, and maintained your skills in medicine as well as possible. Another method would be to enjoy yourself and the break from training, take care of the sailors at your command, and focus on being an exceptional Naval Officer.
If you want to stay current, there is limited funding from BUMED for physicians stationed at non-BSO-18 commands to attend conferences. There are also opportunities for permissive TAD for the purpose of educational opportunities that are advancing of your skills but not necessarily for your command. Moonlighting is also possible with specific permission from the CO and a state license (see MANMED and your local JAGyou’re your moonlighting instruction). Specialty specific resources are available, and you should seek out those from leaders/contacts in your chosen specialty. The UMO tour is a good time to shadow physicians in your specialty, attend academic conference (if feasible), and demonstrate sustained interest. Nearby MTFs can be useful places to stay involved, and there is often command support for maintaining relationships with local MTFs for the purpose of staying current.
UMOs tend to match well for competitive specialties as we tend to be motivated, self-starters with “fleet time” that is highly regarded on GME applications. If you are unsure of making the Navy a career, you can complete four years of HPSP obligation with one UMO tour and attempt to match in a civilian residency. You will have military experience and maturity when matching to civilian residencies; however, you will be somewhat older than your classmates and may need to repeat an internship (depending on which specialty you choose). Whether matching civilian or military, you have a lot going for your application, but without displaying interest in some fashion it can be challenging to match.
HYPERBARICS FELLOWSHIP:
If you desire further training in diving and hyperbaric medicine, you can apply for a fellowship in hyperbaric medicine. This gives you more exposure to the hyperbaric side of the specialty (the Navy training weighs more heavily on dive medicine), opens senior UMO billets up to you, and gives you an additional skill for transition to civilian life. The major locations for fellowship are University of California, San Diego, Duke University (Durham, NC), and Louisiana State University (New Orleans, LA). They typically last for one year and are a good opportunity to get paid a full-time Navy salary while “playing civilian.” If interested, seek out fellowship-trained UMOs for specific details. Of note, in order to qualify for a fellowship, you must be residency trained in a primary specialty. Typical primary specialties for hyperbaric fellowship are Emergency Medicine, Anesthesia, and Primary Care (IM/FP). In order to be competitive for selection by the Navy, you will need to have your Submarine Medical Warfare qualification as well as board certification in your primary specialty.
SENIOR UMO TOUR:
As with all operational medicine tours, there are opportunities to return to the community to serve in a senior UMO role. Group level billets exist for submarines and EOD as well as SMO billets at NSW commands. Some senior jobs require the hyperbaric fellowship (NDSTC, NAMI, NEDU), but most are open to any senior UMO. Most specialties will require a utilization tour in that specialty prior to embarking on a senior UMO tour. You must communicate your desire to leave your primary specialty with your Specialty Leader, be granted authorization to leave the specialty for a tour, and plan on returning to your primary specialty after your UMO tour. These jobs typically involve meetings, medical admin, setting policy for subordinate units, as well as medical oversight of junior medical officers and IDCs. If ultimately interested in this type of role, completing the Submarine Medical Officer Qualification while a junior-UMO is highly encouraged (if not required).
UNIQUE TRAINING OPPORTUNITIES:
- SAT DIVING/AQUARIUS: While the saturation diving program has not been functioning for some time, there has been an effort to revive the Saturation Fly-Away Diving System (SAT FADS), a mobile saturation diving unit built to sustain 6 divers to depths of 1,000fsw for 21 days with 9 subsequent days of decompression. Similarly, the US Navy has had a relationship with the Florida International University Aquarius program, an underwater habitat for saturation diving that has utility for human physiology studies as well as USN training. Introduction to these fields usually starts with a saturation diving course, which runs intermittently at NEDU; contact the UMO at NEDU for more information.
- Dry Deck Shelter (DDS): The US Navy supports Dry Deck Shelter (DDS) operations for launching and recovering of Navy Personnel, SEAL Delivery Vehicles, and Underwater Unmanned Vehicles from Submarines. Training in DDS operations happens intermittently, and can be coordinated with the UMOs at the Seal Delivery Vehicle Team 1 in Pearl Harbor, HI or via Naval Special Warfare Group 3.
- BIENNIAL ICEX: The US Navy does biennial ICE Exercises (ICEX) for evaluation of US Navy Submarine readiness in the unique environment of the Arctic. This is a multinational effort, which allows for multiple UMOs to be involved in either ICE Diving or submarine operations in the arctic. These are extremely unique opportunities only offered to UMOs, and more information can be found via the Arctic Submarine Laboratory (ASL) or the Underwater Warfighting Development Center (UWDC). These operations happen on even years.
- ICE DIVING: The cold water/ice diving course is a course designed to teach you the basics of setting up a dive side on the ice, diving in cold water environments – including the use of a dry suit – and managing the dive side in this environment. This course is offered by the Coast Guard and attended by Navy personnel.
Call for 2020 SECDEF Executive Fellows – O5/O6
The NAVADMIN that announces this program mentions multiple fellowships, but Staff Corps officers are only eligible for the Secretary of Defense Executive Fellowship. Here’s the link:
https://www.public.navy.mil/bupers-npc/reference/messages/Documents/NAVADMINS/NAV2019/NAV19171.txt
Finance Friday Articles
Here are this week’s articles:
6 Reasons Index Funds are King
Add-On CD As A Hedge For Lower Interest Rates
Alpha Investing – An Introduction
Cut Stocks or Add to Them? A Key Dilemma for Your Retirement Plan
Different Ways to be Rich in 2019
Don’t Rely On Predicting The Future
Early Retirement Checklist Part One: Money Considerations Prior to FIRE
Financial Advice Isn’t a Profession
How To Figure Out Your Financial Freedom Number (and What To Do Next)
Is it Wrong for Doctors to Retire Early?
Searching For Happiness When Financially Independent
The Case Against Resident Homeowners
Zero to Freedom Through Cashflowing Rentals (A Course Review)
Throwback Thursday Classic Post – Basic Anatomy of a FITREP
There is a HUGE knowledge deficit in the Medical Corps about FITREPs, which is sad when you consider that they are probably the most important document in our Naval careers. To address this deficit I created this video podcast. In 43 minutes you’ll know just about everything that you need to know about FITREPs. This material is based on about 10 lectures I collected over the years and is consistent with the 2015 update of the FITREP instruction.
Grab a FITREP to look at or start up NAVFIT98a and write your FITREP as you watch the video because it will be much easier to follow along this way. In addition, here are the slides to download and view and the page with all my FITREP resources:
Joel Schofer’s FITREP Prep Page
U.S. Navy Surgeon General Visits Europe to Discuss Readiness and Medical Health Care Transition
WASHINGTON (NNS) — Vice Adm. Forrest Faison, Navy surgeon general and chief, U.S. Bureau of Medicine and Surgery discussed the future of Navy Medicine, and plans to prepare medical personnel for the next fight, while visiting Rota, Spain, and Naples and Sigonella, Italy, July 17-23.
Faison, accompanied by Force Master Chief Hosea Smith, Hospital Corps director, spoke with leaders and Sailors at Naval Hospital Rota, Naples and Sigonella about important changes occurring within the military health system, in particular the transition of all military treatment facilities (MTFs) to the administration and management of the Defense Health Agency (DHA).
“These changes that are occurring,” said Faison, “will allow Navy Medicine to shift our focus from managing buildings and health care benefits to ensuring its people, doctors, nurses, and hospital corpsmen have the skills and experience to keep Sailors and Marines, healthy, ready, and on the job. This transition will allow us to promote Navy Medicine readiness across the world.”
During the multi-day trip, Faison had the privilege to conduct facility tours, admiral’s calls and leadership briefings.
“There is no greater responsibility than then to provide a highly trained medical force that is ready and prepared to save the lives of our nation’s armed forces,” Faison said. “We had a 97 percent survival rate coming out of Iraq and Afghanistan, the highest in all our history, and we had every conceivable advantage, including uncontested air superiority, aeromedical evacuation on demand, seamless communications, and our hospital corpsman, the most important asset on the field.”
Faison explained these advantages may not exist in the next conflict if adversaries are near-peers who can also project sea power. That’s why Navy Medicine has to be prepared for a very different threat and challenge.
Partnerships that prepare Navy Medicine’s Sailors for future conflicts can build on the successes of existing ones, such as Hospital Corpsman Trauma Training, a Navy Medicine program where hospital corpsman have gained hands-on trauma experience at John H. Stroger Jr. Hospital of Cook County, and the University of Florida Health Jacksonville.
“We must show that we are worthy of the trust that is placed in our hands,” said Faison. “We are the ones that care for the 1% of individuals that freely volunteered to uphold our freedom and democracy of this land, and we will do whatever we can to help these military members carry on, in order to defend this country and return them home to their loved ones.”
Navy Medicine is a global health care network of 63,000 personnel that provide health care support to the U.S. Navy, Marine Corps, their families and veterans in high operational tempo environments, at expeditionary medical facilities, medical treatment facilities, hospitals, clinics, hospital ships and research units around the world.
July Message from the Principal Deputy Assistant Secretary of Defense for Health Affairs
MHS Team,
The Military Health System (MHS) continues implementing FY17 and FY19 NDAA-directed reforms – planning and executing the most significant changes to the military medical enterprise in decades. These reforms are looking at different areas of the MHS, from the way we manage healthcare services, to the infrastructure and staffing capacity of Military Treatment Facilities (MTFs), to the broader manpower structure enabling the best possible support to the readiness and lethality of the Department and the National Defense Strategy. While each reform area is distinct, together, they will modernize our approach to military medicine to establish an even more effective, integrated system of health and readiness to support the warfighter and care for the patient.
FY17 NDAA Section 702 will enhance the effectiveness of the MHS by transitioning administration and management of the MTFs from the Military Departments to the Defense Health Agency (DHA). In essence, we are merging four separate healthcare delivery systems into one, consolidating for ease of beneficiary access to high-quality care and standardizing processes and procedures. This will ensure a consistent patient experience at any one of our MTF’s – from appointment scheduling to streamlined referral processes, with standardized performance management systems to monitor readiness, health, access, quality, safety, and cost – and, in turn will enhance clinical competency to ensure a ready medical force and a medically ready force. Last October, eight large MTFs and their associated clinics transitioned to DHA. October 1, 2019 is another major milestone as more MTFs will come under DHA.
One of the provisions in NDAA 2017 requires the Department to conduct a review of the Direct Care System to ensure that MTFs are operating in support of their missions as training platforms for military medical personnel and supporting the medical readiness of operational forces. This review is in its final phase and has included on-site evaluations of select MTFs and assessments of the capabilities of local health care systems to absorb care from the MTFs. Conclusions from these evaluations are being reviewed by senior leaders who will make recommendations to the Secretary of Defense for identification of MTFs for transition to increase or decrease capabilities. The Department will submit a report to Congress outlining recommended MTFs for transition. Facilities designated to transition would begin in FY2020 and could extend through FY2022, depending on transition and local healthcare system expansion timelines. Prior to any change, Congressional notification will be completed in accordance with statute. This reform effort is distinct from MTF consolidation; we are looking at the structure and needs to advance the MHS’s highest priority: to ensure medical forces are ready to support combat forces downrange, and that we continue to build and sustain a world-class health care system geared toward ensuring a medically ready force.
Finally, in order to best support the National Defense Strategy, the Department is comprehensively analyzing medical manpower requirements to meet operational requirements. The Military Departments have recommended force changes based on manpower needed to achieve operational needs. Health Affairs, the DHA, and the Military Medical Departments continue to work closely, developing staffing plans that would achieve the highest readiness and quality of care standards for the warfighter and patient. This effort illustrates the MHS’s inextricable link to the Department’s priorities guiding our strategic direction: getting the military medical force structure right means optimizing personnel, resources, and most importantly, building lethality and support of the force in lockstep with the National Defense Strategy.
While MHS reform brings incredible change, it’s not our only area of focus. We also have new tools at our disposal to deliver on our mission. Next week, I’ll be joining hundreds of uniformed, civilian, contract, and vender experts at the Defense Health Information Technology Symposium (DHITS) in Orlando to talk about how the new MHS GENESIS electronic health record advances readiness, with preparation underway for deployment at Naval Air Station Lemoore, Travis Air Force Base, Army Medical Health Clinic Presidio, and Mountain Home Air Force Base this fall. MHS GENESIS remains a key priority, enabling easier monitoring and response to patient health through an enhanced set of tools to capture the readiness of MHS personnel and service members. The EHR also will improve the way we serve our beneficiaries, whether military members, retirees, or family members.
It’s a productive time for the MHS, and I am grateful for your continued commitment to deliver on our mission. Earlier this week, I joined the 120th Veterans of Foreign Wars (VFW) conference in Orlando to speak with beneficiaries about some of the major MHS transformation efforts underway. I reinforced that while change can be difficult, it also provides the MHS great opportunity to identify innovative ways to more effectively carry out our responsibilities. No matter the organizational reform or change developments to the way we do business, our work together as a team is setting up the future military medical enterprise for success. Keep up the great work!
Tom
