Promotion Boards
Did You Really Fail to Select for Promotion?
If your name was not on the promotion list, you probably weren’t selected for promotion. There is, however, a chance that you actually were selected for promotion but your name was removed after the promotion board. Why would this happen?
After promotion boards there are some systems that are “scrubbed” to ensure that no adverse or reportable information exists for the officers selected by a promotion board or by an administrative board (the CO/XO/CMO/OIC board, for example). Here is a chart that shows you the systems that are checked:

As you can see, if you have problems with your security clearance, the Inspector General, Naval Criminal Investigative Services, or any legal issues, your name could be removed and your promotion put on hold. How do you tell if this happened to you?
First, go to BUPERS On-Line and click on the link for “Advancements/Selection Boards” as pointed out with the large arrow:
Now you should see a screen similar to this one:

As you can see, I was a “SELECT” for O6. If you actually were a non-select for promotion you’d see a “N” where my “S” is. If you were “scrubbed” from the promotion list, you’ll see an “H” for HOLD.
If you don’t see anything, then you didn’t fail to select. You probably weren’t looked at by the board. This most often happens to people who trained in the NADDS program in civilian training programs and weren’t on active duty for a whole year. Sometimes, though, these people will show up on the reserve promotion lists, so don’t lose hope until you check that list as well. As of now, the FY19 LCDR list for the reserves isn’t out yet.
If you are on hold, I’d contact your Detailer to try and find out why.
FY19 Active Duty LCDR Staff Corps Selections
UNCLASSIFIED
ROUTINE
R 231447Z AUG 18
FM SECNAV WASHINGTON DC
TO ALNAV
INFO SECNAV WASHINGTON DC
CNO WASHINGTON DC
CMC WASHINGTON DC
BT
UNCLAS
ALNAV 060/18
MSGID/GENADMIN/SECNAV WASHINGTON DC/-/AUG//
SUBJ/FY-19 NAVY ACTIVE-DUTY LIEUTENANT COMMANDER STAFF CORPS SELECTIONS//
RMKS/1. I am pleased to announce the following Staff Corps Officers on the
Active-Duty list for promotion to the permanent grade of Lieutenant
Commander.
2. This message is not authority to deliver appointments. Authority to
effect promotion will normally be issued by future NAVADMINs requiring
NAVPERS 1421/7 preparation and forwarding of document to PERS-806.
3. Frocking is not authorized for any officer listed below until specific
authorization is received per SECNAVINST 1420.2A.
4. For proper alphabetical order read from left to right on each line.
The numbers following each name indicate the relative seniority among the
selectees within each competitive category. Members are directed to verify
their select status via BUPERS Online.
Medical Corps
Adams Jacob Alan 0028 Adomako Rees Opuni 0247
Ajero Teddy G Jr 0062 Alderson Lauren M 0200
Alex Aea Cowan 0225 Allen Rebecca Melody 0155
Allen Scott Thomas 0090 Anderson Danielle C 0206
Anderson Sarah L 0074 Archer Benjamin James 0073
Austin Ryan Patrick 0099 Bacho Cristina Jean 0190
Balboni Alanna Brooke 0097 Barbante Kathryn R 0072
Barbour Brent Marcus 0080 Barrena Benjamin G 0224
Barrick Clete W 0188 Bartlett Jonette Marie 0186
Bauer Elizabeth May 0032 Bautz Joshua Thomas 0221
Baxter Michael Charles 0226 Bedle Margret Emil 0175
Biscotti Matthew T 0038 Blais Felicia Ashley 0127
Blanchet Scott Michael 0050 Bliss Dani Christine 0002
Bloom Adam Scott 0207 Blum Christina Lahti 0113
Bonds Katherine Annie 0121 Bongiorno Michelle A 0238
Bramble Rebecca Lee 0174 Briden Danielle Amanda 0213
Brisson Jonathan J 0146 Brown Emily Stewart 0199
Brown Jonathan Casey 0164 Buabeng Kwame 0219
Burns Brittany Rose 0177 Bush Allison Marie 0151
Byrne Susanna Martha 0069 Cadotte Noelle Blake 0241
Campbell Paul Charles 0118 Cancian John Wunn 0220
Carr Matthew Joseph 0101 Case Matthew George 0228
Chin John Chui Chung 0001 Chiong Oliver Jeffrey 0085
Cihlar Joseph C 0048 Condos Amy Marie 0100
Condos Gregory Joseph 0098 Contestable James J 0091
Cornell Amy Blackinton 0117 Cowan Wesley Charles 0246
Croom Emily Andrews 0082 Curry Brian Patrick 0149
Daher Dian Krystle 0179 Dangvu Milan Do 0194
Delahanty Liam Francis 0089 Dennig Sean Michael 0116
Dingle Marvin Edward 0010 Dion Suzan Eileen 0066
Donaldson Alana Rae 0165 Dougherty Brian P 0006
Dryden John Randolph 0017 Due April Renee 0122
Elakkad Samih Ehsan 0161 Elsbree Kayleen Ellen 0152
Engle Donald Charles 0003 Espinoza David 0211
Everett Kimberly Ann 0158 Farfan Juanita E 0039
Faubel Kenneth R 0176 Fiacco Nicholas Ryan 0029
Field Robert Dustin 0105 Finn Kristin Jean 0054
Fisher James Arthur 0036 Flood Paul Edward Jr 0242
Foley Jennifer Rae 0079 Foley Sean Patrick F 0092
Ford Caitlin Brooke 0040 Ford Sarah Elizabeth 0070
Frankenstein Nicoletta 0223 Fullenwider Charles O 0163
Gilbert Laura Jean 0138 Guajardo Phillip D 0218
Haddad James Dominic 0053 Hadfield Brandon Reed 0043
Haggerty John Tolman 0210 Hall Benjamen Philip 0021
Hammon Laura Joye 0065 Happach Vincenzo Cosmo 0166
Harding Serennah Emily 0141 Harrison James Michael 0237
Healy Nicholas Joseph 0244 Herforth Christine M 0132
Hicks Aaron Blake 0061 Hodge Daniel K Jr 0112
Hogan Andrew Joseph 0068 Hubbard Mark C 0131
Hughes Stephen M 0239 Hughey Scott Bailey 0096
Jamros Christina Maria 0170 Johnson Erik Daniel 0125
Johnston Luke Ryan 0139 Jolicoeur Megan E 0209
Jones Kelly Lynn 0041 Jones Eric P 0076
Joshi Megha R 0172 Katana Vienna Grayce H 0203
Kerestes Nathan Paul 0081 Keys Kevin Thomas 0154
Kim Sang In 0104 Kinderknecht Kyle J 0142
Kirby Hannah Elizabeth 0143 Kizhner Oskar 0094
Klocek Megan Elizabeth 0134 Ko Samuel Ying 0147
Kortman Francisco C 0144 Krause Jeffrey Allan 0005
Kyle Adrianna Isabel 0169 Lail Matthew Joseph 0111
Landon Matthew David 0083 Landry Travis Obery 0004
Leatherman Matthew L 0067 Lee Katherine Jonnie 0245
Lee Steve Gi Won 0055 Livesey Audrey C S 0087
Lloyd Michael L 0007 Lock Donald William II 0215
Lomas Chad Matthew 0120 Long Ann 0202
Lopreiato Nicholas P 0136 Lyle Anne 0140
Macdonald Alec F 0026 Mandia Jeremy Joel 0077
Marrone Tighe Nicholas 0148 Marvin Kastley Margret 0230
Mccain Laura Abigail 0150 Mcclain Paul David 0153
Mcinturff Mark Ohfuji 0106 Mcintyre Jeannette M 0044
Mclendon Robert Brian 0034 Mcnamara Colin Thomas 0201
Mcnicholas James E Jr 0191 Meredith Bryn Taylor 0181
Middendorf Matthew T 0031 Mikals Samantha J 0078
Montoyavillagomez Migu 0024 Moody Aaron Lee 0037
Moore Andrew C 0235 Murphy Christopher M 0051
Nabet Austin C 0182 Nappo Kyle Edgar 0185
Neubauer Daniel C 0234 Neubert Rachel Anne 0187
Nguyen Lan Anh Thieu 0057 Nicolas Samuel Alvin 0102
Northup Megan Renee 0128 Ochs Ryan Thomas 0197
Ouimet Sean Paul 0011 Pacini Anthony Judson 0171
Parenteau Michael A 0123 Parrott Matthew Jay 0231
Payne Maya Elena 0088 Perez Alfredo 0025
Perez Guillermo III 0236 Pertot Elyse Marie 0137
Pham Hy G 0222 Plasse Richard Andrew 0196
Plata Jose Luis G 0019 Prim James Herndon 0183
Pugh Jackson Charles 0063 Rall Cody J 0204
Ramchandar Nanda 0071 Reed Amy Jean 0159
Regan Matthew Francis 0009 Reichlin Katy Marie 0049
Reynaga Roberto Carlos 0008 Richmond Christopher J 0035
Richmond Kelly Morgan 0093 Richmond Ryan R 0240
Rinehart Charles V 0015 Rocco Nicholas Ray 0103
Roderique Joseph D 0232 Rodriguez Stephen E 0189
Rogers Theodore Hewner 0195 Rozycki Stefan Wass 0107
Rubio Laura Renee 0227 Ryabinin Oleg A 0030
Salazar Krystle May 0042 Sara Matthew Robert 0178
Schafer Jeffrey Martin 0033 Schexnayder Brian 0012
Schmiedecke Rudy F 0114 Seales Paul Evan 0020
Seawright Lisa M 0045 Seider Scott William 0162
Selco Mitchell Marc 0198 Shirk Spencer Ellis W 0124
Slama Elizabeth Milne 0058 Slepski Natalie E 0056
Smith Alfred Gordon 0167 Snyder Scott Howard 0130
Spears Thomas Matthew 0115 Spiro Andrew Joseph 0108
Sprague Justine Marie 0086 Stevenson Rachel Ann 0212
Strain Jonathan Eli 0129 Stromsness Christina 0233
Sullivan Mary Ann 0014 Sutherland Jared M 0135
Szatkowski Angela N 0027 Taylor Zachary Andrew 0046
Teisberg Madeline B 0180 Towb Parmalee C 0023
Townsend Cassandra K 0145 Vanbrunt Thomas B Jr 0217
Vanhorne Edgar Myoung 0047 Vantassel Craig James 0192
Vest Ryan Matthew 0095 Vienna Ryan Patrick 0084
Volk Charles Gabriel 0160 Walker Christine Marie 0214
Waller Travis Lee 0018 Walsh James Bernard 0229
Wang Andrew Wilson 0156 Ward Dawn Kabrich 0216
Ward Meghan Nichole 0052 Watters Julie Ann 0110
Wauters Robert Henri 0157 Wheatley Benjamin M 0064
Whitlatch Meghan A 0173 Whittington Julie R 0126
Wilcox Timothy David 0208 Willett Peter Bryce 0075
Wilson Justin Dean 0168 Wingen Elizabeth Anne 0193
Winn Aubrey Elizabeth 0243 Winship Emory S VII 0059
Woelfel Gregory Alan 0013 Wright Andrew Jonathan 0060
Writer James Kendrick 0016 Zenk Reilly Louise 0119
Zitnik Kenneth Erin 0184
Dental Corps
Archer Benjamin Paul 0010 Barrett Jason Lawrence 0020
Barth Christopher T 0044 Berg Rebecca Adeline 0012
Berkowitz Danielle P 0006 Blackmore William S 0043
Boland Kathleen Brigid 0034 Bond Dustin Aldridge 0029
Brewington Ashley K 0046 Burns Krystal Hope 0021
Burr David Parent 0045 Cammack Bradley Kent 0003
Carlo Catherine Eva 0053 Crossland Nicholas F 0058
Defazio Michael Carey 0052 Dickens Noel Evan 0008
Dyer Amanda Nichole 0047 Ellenbecker Tyson A 0025
Engelbrektson Erik A 0032 Eriksson Kurt Allan 0040
Fetters Chase Westhall 0041 Fila Juliana Clove 0051
Flores Broc Antony 0035 Gonzalez Elias Daniel 0039
Greiner John Houston 0031 Heim Eric Peter 0014
Hofferber Craig E 0048 Jakubowicz Phillip A 0005
Jing Wilson Shuaiwen 0022 Kaemmer Ian Jameson 0033
Keener Dylan James 0017 Knofczynski Andrew R 0019
Knudson Andrew James 0042 Krupinski Cathern N 0026
Langenderfer Kurt A 0009 Langkau Walter Samuel 0016
Maghsoodpour Arbel 0038 Maliken Christopher G 0018
Marin Anthony James 0060 Martin Trevy Kyle 0024
Mcginn Mary Catherine 0057 Meadows Coleman D 0004
Neal Russell Lawrence 0011 Parker Taylor Aaron 0013
Pasch Sarah Jane 0030 Perrone Lisa Carol 0050
Roadarmel Stephanie L 0059 Ryan Mark Daniel 0002
Schaefer Lulu Fang 0054 Seywerd Johannes N 0001
Staller Benjamin L 0015 Thomas Stephen Craig 0023
Tran Tuan Ngoc 0056 Urbaitis Michael James 0028
Vertolli Travis J 0037 Way Tyler Scott 0049
Weenig Joshua Ammon 0027 Winks Ryan Joseph 0055
Yang Michael Keene 0036
Medical Service Corps
Agbo William Ayikwei 0008 Aguirre Billy Lemus 0101
Allen Anthony Clark 0130 Allen April Rene 0145
Anderson Eric Edwin 0154 Atterbury Jessica T 0169
Ayeni Temitope Oladipo 0062 Babskie Daniel Andrew 0159
Banker Leticia D J 0082 Banks Ellis Lee II 0087
Barlow James Nathaniel 0041 Becker William F 0010
Bell Maya Naima 0106 Bell Phillip Martin 0151
Bell Steve Jason 0170 Beltran Manuel H 0071
Bencivenga Mario A 0122 Berg Amanda Elizabeth 0045
Berlin David B 0005 Bly Richard J 0051
Boudreaux Amanda Faye 0016 Brower Sarah Joy Han 0162
Brown Lisa Annmarie 0115 Campbell Ariel Reve 0117
Cavallario David James 0065 Chamberlain Derek John 0149
Chavez Francisco R 0004 Collins Michael John 0021
Conboy Christopher Lee 0110 Corbridge Joshua D 0165
Cote Noel Michael 0083 Craig Jennifer Lynn 0072
Crawford Cynthia Beth 0144 Cusack Terence Jose IV 0049
Davidson Brian Scott 0048 Decletwhiting Monica I 0085
Delano John Charles 0058 Desiderio Brian C 0166
Doucette Ari Sean 0119 Edouard Joseph 0015
Elliott Linda Marie 0056 English Erik Lee 0022
Fail Richard Howard 0091 Falkner James Thomas 0133
Frasco Jenny Marie 0038 Fuchs Jason Benjamin 0123
Furnish Lana Michelle 0068 Galassoalexander Vivie 0069
Geeseman Joseph W 0113 George Timothy Lee 0102
Glienke Carl Jonathan 0136 Goebel Neal Christiaan 0148
Golla Stephanie 0050 Gonzalez Nicole K 0059
Gradwell Amelia Grace 0161 Green Shellita Frances 0090
Gregory Pamela K 0129 Guadalupe Nelson H 0073
Guajardo David Daniel 0152 Hartley Clark Kimball 0127
Harwood James Flint 0099 Hayes Selena M 0163
Hester Brandon Jerome 0121 Hill Aaron Jackson 0116
Hine Carolynn Anne 0095 Hoblet Justin Woodrow 0158
Holbrook Brian James 0103 Holland Tamora Leona 0024
Holman Carolyn J 0031 Houston Natasha Mary 0001
Jeanlouis Peter L 0076 Jensen Jason Paul 0141
Johnson Jermaine T 0092 Jones James Kevin 0023
Kaheakuenhada Erika M 0064 Kallail Donald J III 0107
Kelso Michael Gavin 0074 King Taj Dwayne 0025
Knapp Jennifer Alicia 0043 Knorek John Kenneth 0078
Laffman Keith Matthew 0070 Laird Melissa Dee 0126
Lane Michelle Hartman 0061 Larsen James Douglas 0075
Lawson William K Jr 0027 Lea Michelle Ann 0140
Lee Albert Jong Suk 0124 Letizio Samantha Emily 0167
Lockett Sandra 0012 Loe Martha Anne E 0104
Lorenzo Ronald Richard 0028 Macaskill Rebekah Lynn 0029
Matosmakris Nikolas A 0084 Mayr Joseph James 0098
Mccormack Nakima V 0046 Mcguire Patrick Wayne 0063
Mclamb Brandon Odell 0066 Mcveigh Timothy Edward 0039
Meloscia Chantal E 0036 Menck Elisa Sue 0114
Mene Rey Bucol 0080 Messick Michael J Jr 0055
Miller Edward T 0164 Milstein Matthew Evan 0040
Mitchell Patrick James 0168 Mize Kenneth Leon Jr 0134
Morrison Jay Arthur 0125 Mulvey Emily Kay 0112
Musmanno Joseph Hays 0079 Nance Erika Teresa 0054
Naranjo Daniel F 0147 Niven Jason Ryan 0120
Noakes Nathan David 0153 Nyangena Isaac M K 0097
Oakes Jonathan F 0002 Oehrlein Christopher S 0111
Ohaeri Nnamdi Glenn 0033 Oleary Michael Todd 0137
Olson Andrew Spencer 0020 Palmer Jonathan Mark 0128
Pavlicek Rebecca Lou 0018 Pendergrass Jesse Ray 0132
Peters Christopher Y 0088 Petikas Nicholas C 0160
Peugeot Mark David 0006 Pietila Diane Marie 0047
Punzal Jaypee Albano 0037 Qui Harry Zhang 0109
Rakich Danielle Nicole 0060 Randle Derrick Nashaun 0089
Randles Amanda Jane 0053 Reyes Kristoffer Sol B 0042
Ricker Lucas Lance 0093 Rivera Brad Alan 0138
Rosete Arthur Castillo 0003 Rowe Duane Shaw Jr 0150
Ruff Juliette D 0052 Ruppert Arthur Shawn 0135
Russell Brandon J 0030 Sadosky Angela Rose 0142
Sargeant Rachel Marie 0157 Saul Kathleen Mary 0032
Schmitt Stetson Robert 0108 Shenbergerhess Ashley 0035
Siu Fei 0011 Skelton Donald Morales 0094
Smithson William A 0034 Specht Lauren Vaughn 0139
Spellman Tanya Melissa 0131 Steele Michael Caleb 0019
Stephens Kevin R Jr 0026 Stewart Jesse Steven 0086
Strobridge Virgil R 0081 Suszko Christopher M 0057
Tate Kei Amber Juanita 0013 Tomlinson Adam Blake 0077
Tracy Caleb Helaman 0096 Trimner Stacey Marie 0044
Vahamaki Niko Olavi 0009 Vaughan Thomas Daniel 0105
Volk Paula Sue 0146 Vorwald Jeffrey David 0156
Warpula Erick Wayne 0100 Webb Alisha Laray 0007
Wheeler Theodore C 0143 White Veronica Holguin 0155
Whittaker Reginald C 0067 Wilson Sobondo Josiah 0017
Wofford Angela Marie 0118 Wolfley Gregory Alan 0014
Judge Advocate General's Corps
Aliano Adam Corey 0032 Anderson Keleigh 0026
Beard Kathryn Deangelo 0004 Blair Tadd Coles 0011
Breuder Philip Edward 0044 Brookes Warren Leigh 0008
Brown Joseph Striker 0040 Budow Matthew Jaret 0018
Clayton Ashley S 0021 Collett Michael D 0035
Cotten Christin E 0017 Daniels Emily Anna 0031
Duru Omer Jr 0015 Foley John Paul 0039
Gioiello Alexandra J 0034 Gonzales Joanna Maria 0046
Hagedorn Christine R 0025 Harbas Simone Stefanie 0028
Inns Nicholas James S 0003 Jarczyk Elizabeth Jean 0020
John Brian Patrick 0022 Jooshani Sahar 0041
Kiefer Oliver Moody 0043 Kohlhofer Kelly Marie 0007
Lawler Michael Sturgis 0038 Mangual Daniel R 0014
Marcinskas Emil 0030 Marquez Victor Lee 0027
Masterson Jason R 0001 Mcginley Daniel Ryan 0045
Meyer Bradley F 0006 Mooney Ryan Andrew 0010
Morrison William M 0036 Mosimann James E III 0009
Murphy Kymberly Lee 0012 Newsad Bradley Douglas 0037
Nichol Alyssa Kate 0016 Oakes Ann Tuddenham 0019
Obrien Conor Logan 0002 Pehl Shaun M 0013
Reardon Michaela Anne 0024 Riedel Christopher K 0033
Sussman Rachel Faye 0042 Sylvester Ryan James 0023
White John Cherne 0005 Williams Sharlena Y 0029
Nurse Corps
Abadilla Mark Anthony 0100 Acedera Paolo A 0045
Alcantar Marcello A 0085 Allbaugh Matthew 0002
Anderson Sarah Michele 0058 Battle Claudia L 0115
Berger Robert Harold 0095 Bokan Melissa Marie 0108
Bratton Carrie E 0022 Brenes Any 0072
Brion Caitlin B 0087 Brogdon Laurabeth K 0047
Brown Michelle Marie 0082 Bush Sarah Jane L 0055
Caldwell Jason Dean 0080 Chavez Augusta Mary 0083
Cole Francene Elaine 0078 Collazo Christina K 0062
Collins Willie R Jr 0059 Crosby Tatiana 0035
Cummiskey Angela L 0049 Cummiskey David P 0050
Daniell Stephany Jin 0094 Davidson Michael James 0019
Deppen Resel V 0109 Diggs Thomas Lee 0020
Dinan Lauren E 0044 Duncan Kizzy Hope 0014
Echon Jerrieallen F 0116 Edouard Teresa Ann 0074
Edwards David Keith 0063 Evans Shannon Lynn 0064
Evans Tanikka Rashanda 0039 Felipe Anuel 0033
Flores Nita 0024 Folstad Erin Michelle 0089
Fulks Kelly Ann 0093 Gagliano Erin Leigh 0084
Galicinao Gary Tobias 0053 Gemme Jacqueline Marie 0066
Gilliam Joshua Henry 0041 Gonzalez Marissa V 0079
Gorman Jessie Lyn 0011 Haney Kellie Jo 0071
Henry Thomas Michael 0073 Hesse Marissa Alice 0015
Hoff Sharon Margaret 0040 Howell Sierra W 0016
Hull Sarah Kathleen 0096 Jacobs Hadde Elizabeth 0032
James Cylyne A 0034 Johnson Aaron Donald 0086
Johnson Justin Jeffery 0097 Kim Sue Mee 0112
Kretchman Allison Ann 0069 Laccay Gary Oliver G 0007
Lange Joshua Thomas 0081 Lanthorn Michael D II 0054
Lateef Saheed A 0113 Lewis Tarah Bryanne 0036
Manko Logan Andrew 0056 Marashi Zena Parastu 0060
Marsh Rachel Anne 0091 Mattox Patrick Wesley 0061
Mcadams Chaia Elyse 0105 Mccullers Marisa Lynne 0025
Melchi Joseph Alan 0031 Milan Ryanjon A 0101
Miller Jessica Ashley 0004 Mitzkewich Margaret P 0106
Mongeperez Juanmanuel 0008 Mora Ferran 0023
Naranjo Jessica N 0114 Neal Amber L 0046
Panolli Julian 0029 Partner Amanda Maureen 0111
Petersen Neal C 0077 Phillips Jonathan Lynn 0009
Proano Marylou C 0110 Qiu Alexia Marie 0065
Ramsay Kristel Danette 0038 Reese Charlene S 0010
Riffle Jimmie G II 0027 Riojas Francisco G 0030
Rodriguez Gabriel R 0102 Rosholt Stephanie M 0070
Sanchez Eric Alforque 0099 Schuetz Lauren E 0048
Schurman Alison Mary 0001 Shannon Tabitha Sue 0057
Sharp Kelso Eugene II 0017 Sierleja Kenneth F 0042
Sikes Teresa Lynn 0005 Smith Shannon Blue 0037
Snyder Meaghan Rose 0107 Soriano Mark Cristan 0088
Starling Amy Lauren 0067 Stone Liza 0021
Sweeney Sheila A 0052 Tranberg John W III 0098
Troncozo Melissa Kay 0104 Trudell Marshall Aaron 0103
Turner Rita M 0092 Veldhouse Theresa Jo 0028
Vranianwade Jentry E 0003 Waddell Erica Sharice 0076
Walker Fagwenlanita R 0006 Washbon Karri Lynn 0090
Waterfield Lynette M 0013 West Candice Marie 0026
White Rachel Susannah 0068 Wilhelm Shawn Mathew 0117
Wilson Meghann K 0043 Wilson Yolanda T 0012
Yazici Nevin 0075 Yohannan John S 0051
Supply Corps
Adjei Mark 0044 Agojo Michael Mayandoc 0036
Andrews Joshua Adam 0021 Begin Les M 0056
Benavidez Rommel Laylo 0019 Bencs Shannon Kristine 0026
Berry Jonathan Hawkins 0032 Biddle Tyson Matthew 0048
Brenner Ian Andrew 0042 Buensuceso Christian L 0008
Cabe Paul M 0039 Caldwell Gabriel R 0057
Caldwell Marcus Edward 0074 Campbell Margaret M 0045
Carmack Ryan C 0017 Cassady Alexander R 0016
Catacutan Carlisle R 0041 Clark Leslie Ray II 0050
Cline Marcus Russell 0053 Coleman Dustin Todd 0006
Culp Christopher Shawn 0009 Davis Joseph Prentis 0040
Durakovic Asim 0003 Easterling Gregory K 0064
Edwards Paul Anthony 0025 Fish Aaron Brolin 0051
France Wyatt James 0012 Francia David F 0005
Fritsch Robert A 0046 Gage Austin William 0014
Galvan Araceli 0002 Gangcuangco Peter John 0015
Garner Blake Demetrio 0063 George Jason Philip 0072
Greenlaw Seth Damion 0001 Grimes Jacob Matthew 0011
Guillory Hilman I Jr 0075 Harlan Seth Wendell 0024
Harman Daniel Allen Jr 0037 Harvey Christopher J 0035
Hough Keith A 0071 Hughes Jay Harrison 0027
Hunt David James 0020 Jarreau Irina 0030
Julao Jesse Vitug 0065 Kiengsiri Jesse Y 0018
King Bryan William 0059 King Jonathan Robert 0067
Kojm Peter Maximillian 0043 Landon Joseph Michael 0061
Larenas Emma Rachele 0054 Martindale Dustin R 0060
Martorano Eric Carlo 0004 Mercier Sean Philip 0028
Miller Sand Denise 0031 Morris Kiera Marie 0052
Nguyen Thuy Le Thanh 0047 Oliveria Christopher D 0038
Paige Dylan Scott 0022 Park Michael Roy 0034
Petrinovic Jonah A 0023 Routley Robert Damon 0055
Santiago Jeremy R 0066 Seals Jermaine Lovell 0058
Stewart Brandon Allen 0069 Sturgis Bradford R Jr 0068
Styer Varsha 0007 Ta Phuong Anh Chau 0070
Toner Mark Christopher 0010 Traul Jennifer Alison 0073
Turner Rickey 0029 Uyan David Jeremy 0013
Vining Kirk William 0049 Wall Kevin Matthew 0033
Wilder Darian Jovon 0062
Chaplain Corps
Alander Nicholas Loren 0047 Arant Jason Robert 0033
Asbury Brenton C 0015 Black Jonathan C 0002
Box Benjamin Maurice 0031 Brod Andrew Joseph 0026
Burleson Saul Lars 0051 Butts William Daniel 0021
Byrd Lara Caulder 0029 Carson Philip David 0024
Choi Jin 0030 Chung Daniel Eun 0044
Coffey Travis Edward 0038 Craig Barrett David 0028
Crone Loren Michael 0007 Drayton Matthew W 0036
Fore Matthew Churho 0019 Francis Andrew Maynard 0052
Freiberg Shane Matthew 0042 Grant Aman Joseph 0035
Harris Matthew Arthur 0032 Hayes Justin Michael 0018
Henderson Jonathan M 0046 Hervey Steven Glenn 0054
Hood Brandon Keith 0001 Horn Jessica Katherine 0025
Jones Reginald Earl Jr 0048 Labue Stephen Anthony 0020
Lightner Keith Jerome 0055 Lim Kevan Qinxin 0053
Lurer Amanda Rachel 0050 Mallie Charles Stephen 0041
Mcgraw Eamon Allen 0045 Mcmurry Doyl Emory 0009
Miller Baron Clint 0034 Neil James Jonathon 0005
Pepper Gary Welter 0010 Phelps Flournoy Casey 0016
Price Robert Charles 0013 Quay John Mark 0022
Rice Nathan Neil 0023 Sanders Nashaunna S 0004
Schumann Paul Andrew 0049 Scott Stephen Robert 0037
Shepard Matthew Dean 0040 Sluder Jason Bradley 0011
Smith Jared Nathaniel 0006 Taylor Kendall Wayne 0012
Trumble Todd Andrew 0017 Um Junsub 0003
Walker Steven Michael 0039 Weikel Ralph M Jr 0027
Wilkinson Kevin Scott 0008 Williams David Ryan 0043
Williams Patrick Devon 0014
Civil Engineer Corps
Bessette Andrew Paul 0007 Bozek Michael Edward 0012
Brown Forrest A 0009 Chase Carl Cline III 0026
Cloutier Daniel D 0037 Cuevas Raul Eduardo 0001
Deiuliis Peter James 0014 Doe Kevin Kai Fung 0002
Doyle Ryan Taylor 0027 Dreyer David Madison 0035
Duffy Michael J 0019 Eberhart Michael B 0021
Feeney Michael James 0034 Griffin Arthur Eugene 0025
Hall Joshua Alexander 0016 Herm Kimberly A 0015
Mack Brian Glenn 0006 Martinez Christian U 0011
Myers Travis Rea 0024 Obasi Taibatu E I 0010
Orr John Patrick 0018 Parizek John Michael 0032
Pasteur Don 0028 Pine Matthew Alan 0005
Riege Matthew Kyle 0033 Smith Jeremiah Patrick 0020
Sovie Alexandria Mae 0023 Strausbaugh Kyle P 0022
Tatel Samuel C 0017 Thomas Christopher A 0003
Thompson Robert John 0036 Ward Mathew James 0030
Webb Justin Pat 0031 Wijas Michelle T 0004
Willich Christopher M 0008 Wise Oliver James 0029
Worthington Stanley R 0013
Limited Duty Officer (Staff)
Alshabazz Albetro 0003 Thomas Dewayne Alan 0001
Wood Brian Michael 0002
5. Released by the Honorable Richard V. Spencer, Secretary of the Navy.//
BT
#0001
NNNN
UNCLASSIFIED//
Navy Times – Congress, Navy Revolutionize Officer Promotions
Here’s a link to this interesting article:
Military Times – Pentagon Braces for Massive Change to Officer Promotions
Here’s a link to this article:
Officer Promotions and the NDAA 19
Physicians are always interested in promotions, and the proposed NDAA 19 makes a number of changes to officer promotions. If you want the scoop, first I’d read this article from Military Times:
Congress is Giving the Officer Promotion System a Massive Overhaul
In addition, here are the relevant changes I pulled out of an article from the DHA Early Bird a few days ago:
- Officers will continue to be considered for promotion as part of the same year group in which they were promoted to their current rank.
- Congress is required to annually authorize the number of officers allowed to serve in the ranks of O4 through O6 across all the services.
- It repeals a requirement that candidates for regular commissions not be older than 42, or at least have enough service years to complete 20 years by age 62.
- It enhances the services’ authority to award constructive service credit for special private sector training or experience to allow active or reserve officer appointments up to the rank of O6 in critically needed fields.
- Authorizing each service to award temporary promotions to the ranks O3 through O6 for specified positions. Only Navy has such authority today so this change would standardize it across all branches.
- Authorizing promotion boards to recommend that “officers of particular merit” be placed higher on promotion lists than peers.
- Allowing officers, when deemed in the best interest of the service, to have their names removed from consideration by a selection board for promotion to the next higher grade, and authorizing officers in certain military specialties to remain on active duty until reaching 40 years active service.
- Authorizing use of an alternative promotion processes for officers in certain secretary designated competitive categories, to include a term based continuation process when certain officers are not selected for promotion. This would selectively end the traditional up or out requirement for officer management.
The devil’s in the details, and the Military Times article states that the changes are not mandatory for the services, so we’ll have to see how it all plays out over the next few years.
FY19 Medical Corps O5 Promotion Stats
| FY19 MEDICAL CORPS COMMANDER SELECTION BY SUBSPECIALTY | |||||||||
| SELECTION OPPORTUNITY 85 % | |||||||||
| # IZ | #SEL IZ | % SELECT IZ | # AZ | #SEL AZ | % SELECT AZ | # BZ | #SEL BZ | % SEL BZ | |
| FLT SRG | 2 | 0 | 0.00% | 4 | 0 | 0.00% | 11 | 0 | 0.00% |
| RAM | 3 | 1 | 33.33% | 9 | 1 | 11.11% | 5 | 0 | 0.00% |
| ANESTH | 12 | 6 | 50.00% | 9 | 5 | 55.56% | 23 | 1 | 4.35% |
| SURG | 20 | 11 | 55.00% | 15 | 7 | 46.67% | 34 | 0 | 0.00% |
| NEURO SURG | 6 | 1 | 16.67% | 1 | 1 | 100.00% | 5 | 0 | 0.00% |
| OB GYN | 8 | 4 | 50.00% | 10 | 6 | 60.00% | 11 | 0 | 0.00% |
| GMO | 2 | 0 | 0.00% | 2 | 0 | 0.00% | 9 | 0 | 0.00% |
| OPHTH | 3 | 1 | 33.33% | 1 | 1 | 100.00% | 2 | 0 | 0.00% |
| ORTHO | 13 | 8 | 61.54% | 5 | 2 | 40.00% | 26 | 0 | 0.00% |
| OTO | 6 | 5 | 83.33% | 4 | 3 | 75.00% | 6 | 0 | 0.00% |
| URO | 2 | 2 | 100.00% | 1 | 0 | 0.00% | 8 | 0 | 0.00% |
| PREV MED | 2 | 2 | 100.00% | 7 | 2 | 28.57% | 2 | 0 | 0.00% |
| OCC MED | 3 | 1 | 33.33% | 4 | 1 | 25.00% | 6 | 0 | 0.00% |
| PHYS MED | 2 | 0 | 0.00% | 0 | 0 | N/A | 1 | 0 | 0.00% |
| PATH | 3 | 2 | 66.67% | 6 | 2 | 33.33% | 4 | 0 | 0.00% |
| DERM | 5 | 2 | 40.00% | 1 | 1 | 100.00% | 11 | 0 | 0.00% |
| EMERG | 10 | 3 | 30.00% | 9 | 6 | 66.67% | 30 | 0 | 0.00% |
| FAM PRAC | 18 | 5 | 27.78% | 16 | 7 | 43.75% | 51 | 0 | 0.00% |
| INT MED | 17 | 12 | 70.59% | 18 | 5 | 27.78% | 36 | 0 | 0.00% |
| NEURO | 0 | 0 | N/A | 0 | 0 | N/A | 6 | 0 | 0.00% |
| UMO | 1 | 1 | 100.00% | 3 | 1 | 33.33% | 5 | 0 | 0.00% |
| PEDS | 10 | 7 | 70.00% | 6 | 2 | 33.33% | 16 | 0 | 0.00% |
| NUC MED | 0 | 0 | N/A | 0 | 0 | N/A | 0 | 0 | #DIV/0! |
| PSYCH | 9 | 7 | 77.78% | 4 | 1 | 25.00% | 19 | 0 | 0.00% |
| DIAG RAD | 15 | 8 | 53.33% | 12 | 1 | 8.33% | 21 | 0 | 0.00% |
| RAD ONC | 1 | 1 | 100.00% | 2 | 1 | 50.00% | 3 | 0 | 0.00% |
| TOTAL | 173 | 90 | 52.02% | 149 | 56 | 37.58% | 351 | 1 | 0.28% |
| FY19 MC CDR SELECTIONS BY ZONE | |||||||||
| # OF PEOPLE | # SELECTED | % SELECTED | |||||||
| ABOVE ZONE | 149 | 56 | 37.58% | ||||||
| IN ZONE | 173 | 90 | 52.02% | ||||||
| BELOW ZONE | 351 | 1 | 0.28% | ||||||
FY19 O4 Medical Corps Promotion Opportunity is 100%
As usual, the O4 promotion opportunity for Medical Corps officers is 100%. How do I know? Because the day the board starts you can go to the board webpage, download the convening order, and check page 2. It is always there.
Here’s the website:
http://www.public.navy.mil/bupers-npc/boards/activedutyofficer/04staff/Pages/FY-19.aspx
Here’s the convening order. Check page 2:

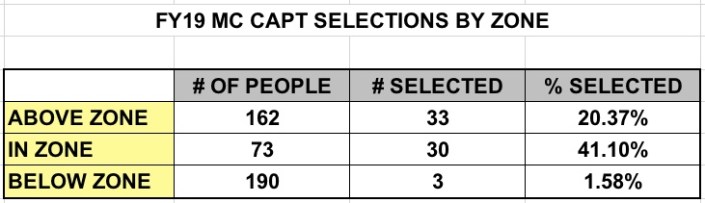
FY19 O6 Staff Corps Promotion Board Statistics
The Medical Corps statistics were:
- Above Zone: 33 selected of 162 eligible = 20.4%
- In Zone: 30 selected of 73 eligible = 41.1%
- Below Zone: 3 selected of 190 eligible = 1.6%
- Total Selected = 66
The other staff corps board stats can be found in this document:
