Update on DHA Transition in June Message from the Principal Deputy Assistant Secretary of Defense for Health Affairs
MHS Team,
As the Military Health System (MHS) has continued implementation of FY17 National Defense Authorization Act (NDAA) Section 702, we’ve revised our approach for transitioning administration and management of the Military Treatment Facilities (MTFs) from the Military Departments to the Defense Health Agency (DHA). Our original implementation framework required maintaining Military Department Headquarters and Intermediate Management Organization (IMO) MTF management responsibilities for an extended period of time to support those MTFs in geographic regions as we phased in MTF transfers to the DHA over several years. Recognizing this approach had several challenges in addressing civilian personnel changes, financial resources, and the Military Departments’ ability to focus on medical readiness, in May the MHS leadership team recommended a new transition framework to DOD and Military Department senior leadership. Our new framework has DHA assuming authority, direction, and control of all MTFs on October 1 of this year and DHA will oversee the MTFs through a Direct Support relationship from Military Department IMOs. The DHA will relieve the Military Departments of this support during a transition period during which responsibility for specific functional capabilities are fully transferred from the Military Departments to DHA under a controlled “hand off.” For the remainder of FY19, the DHA and the Military Departments will finalize and implement the necessary memoranda of agreement to formalize this Direct Support approach.
At the same time, our work to carry out FY17 NDAA Section 703 continues as we prepare to adjust the MHS infrastructure to better support operational readiness requirements. Over the past several months, OASD/Health Affairs-led teams have conducted site visits to dozens of facilities, assessing both “on base” health services and needs, as well as the capacity of nearby civilian networks. The goal is to complete a top-to-bottom review of MTF capacity to ensure we dedicate the right personnel and resources to meet readiness requirements and identify any insufficient network coverage for our 9.5 million beneficiaries. To date we’ve identified 73 MTFs that merit additional analysis, and we are working to provide a final report and recommendations to Congress later this summer.
The Department continues to assess the medical manpower requirements in support of the National Defense Strategy. The Military Medical Departments have put forward their recommendations for force changes based on operational requirements, manpower needed, and subsequent proposed manpower reductions. Health Affairs, the DHA, and the Military Departments continue to work closely together to implement the medical force changes to meet future operational requirements while ensuring the MHS continues to provide the highest quality health care services possible to our patients.
Amidst these major organizational changes, our colleagues across the MHS continue to support medical operational requirements and deliver outstanding medical care to service members, retirees and their families. Earlier this month I had the opportunity to see firsthand evolving capabilities of the MHS when we visited Nellis and Creech Air Force Bases, Nevada. The trip illustrated how greater integration of services between the Military Health System, VA and local health systems can strengthen readiness support to the combatant forces and the delivery of quality care to the entire beneficiary population. I had the honor to meet with several military unit commanders and their staffs including: The 99th Medical Operations Squadron (99th MDG) at the Mike O’Callaghan Military Medical Center; 66th Rescue Squadron; 57th/757th Aircraft Maintenance Squadron (AMXS); Creech Medical Clinic; and the 42d Attack Squadron (42 ATKS) and 42d Attack Squadron-Human Performance Team (HPT). I toured the Reaper Operation Center (ROC) Orientation & Ground Control Station (GCS) where General Hogg, Air Force Surgeon General, and I had the rare opportunity to fly a Remotely Piloted Aircraft mission in the flight simulator.
Rounding out the time with the Air Force components was the opportunity to visit the University Medical Center (UMC) to learn about the benefits of the Nellis partnership with this leading Las Vegas provider. Through this partnership Air Force physicians, nurses and technicians are able to temporarily work and train at UMC of Southern Nevada to help ensure they stay current and maintain the highest levels of readiness.
Last month, Dr. Terry Rauch, Acting DASD Health Readiness Policy and Oversight and our Global Health Engagement team participated in the 43rd International Committee on Military Medicine World Congress in Basel, Switzerland. Since 1921, the ICMM has worked to strengthen cooperation between the health services of militaries worldwide. The United States is proud to be one of the founding members of the ICMM, and U.S. military medicine remains committed to this enduring partnership as we step into the Vice Chair role. That commitment is fully in keeping with one of the pillars of our National Defense Strategy, which calls for strengthening our existing global partnerships and seeking to work with new partners.
Back at the Pentagon, the Health Affairs team bid farewell to COL Jesse Ortel, CDR Tilford Clark and LCDR Kishla Askins. A special thanks to these exceptional staff members for their significant contributions and unwavering dedication to the Health Affairs team over the past years. I wish them all the best in their future endeavors. As they depart, we are pleased to hail the newest members to Health Affairs: COL Chris Warner, Military Deputy and Chief of Staff; LCDR Chris Barnes, Military Assistant; LT Ariel Campbell, Deputy Director for MHS Governance/Integration Officer; Dr. Jill Sterling, Program Director, Medical Quality Assurance and Clinical Quality Management Policy; and Dr. Richard Mooney, Director of Health Services Policy and Oversight. Welcome to the team!
Lastly, I’d like to recognize our MHS Communications Team for winning the prestigious Silver Anvil Award from the Public Relations Society of America, as well as the Hermes Creative Award for the Take Command campaign executed last year to inform TRICARE beneficiaries about the many changes to their benefit. Congratulations on this great achievement – a true testament to the MHS’s commitment to meeting the needs of our beneficiaries.
Navy Announces Spouse Licensure and Certification Reimbursement Policy
Here’s a link to this blog that probably affects a lot of my readers:
Navy Announces Spouse Licensure and Certification Reimbursement Policy
Cheaper SGLI and Finance Friday Articles
I always read my military pay stub, the Leave and Earnings Statement or LES. This month it said:
THE SERVICE MEMBERS GROUP LIFE INSURANCE AND FAMILY SGLI PREMIUM RATES WILL BE REDUCED EFFECTIVE 1 JULY 2019. THIS WILL LOWER PREMIUM RATES FOR ALL SERVICE MEMBERS. FOR NEW RATES VISIT: HTTPS://WWW.BENEFITS.VA.GOV/INSURANCE/SGLI.ASP
My SGLI of $400,000 just went from $29 per month to $25 per month. If you click on the link above, you can see the old and new rate tables.
Here are this week’s articles:
7 Ways the Rich Pay Less in Taxes (and You Can Too)
25 Best Personal Finance Blogs (Why You Should Read)
Don’t Buy Stuff You Can’t Afford
Don’t stop believing in the benefits of indexing
Do What You Want When You Want To
How Do Financial Advisors Get Paid – A Financial Planner’s Perspective
How to Get Rich: Curbing Spending on the Big 5
How to Win Any Argument About the Stock Market
This is Why Tax-Efficient Investments Are Important
Top 5 Reasons Tracking Spending is Problematic
Where’s the Value? A Discussion About Value Tilting Your Portfolio
Throwback Thursday Classic Post – How to Manage Your PRD and Not Get Stuck with a “Hotfill”
(I’m going to start re-posting some of the better and more popular blog posts on the site on Throwback Thursday. Much of the content is evergreen or requires minimal updates, and the blog has a much larger readership than when many of these posts first ran.)
There are many important dates in your Navy career. One of the most important and neglected dates, though, is your projected rotation date or PRD. Your PRD is the month and year that your current orders will expire and you are scheduled to rotate to a new command. If you don’t manage your PRD and pay close attention to it, you can find yourself with few career options and in a situation you never thought you’d be in. With that in mind, here are my tips for managing your PRD.
Know Your PRD
First, know when it is because many physicians don’t know their PRD. If you are in this crowd, the easiest way to find your PRD is to login to BUPERS On-Line and look at block 14 of your Officer Data Card:
The other way to find your PRD is to contact your Detailer because they can look it up in the detailing system. Many physicians don’t know their Detailer, so here is a link to a page with “Contact Us” in the middle.
Manage Your PRD
Once you know your PRD, the easiest way to manage it is with whatever calendar you use (an app, web calendar like Google Calendar, Outlook, a date book, etc.). Place reminders in your calendar to correspond with these time frames:
13-18 Months Before Your PRD – This is when you should start thinking about your next career move. Although the normal time period to request an extension (find a template here) at your current command is 9-12 months before your PRD, many physicians request an extension during this time period if they are sure they want to extend. This is also a great time to talk to the Operational Detailer about operational billets you might have interest in or the Senior Detailer about what I’ll call “alternative billets” like those at DHA/BUMED, BUPERS, global health engagement billets, NAVMEDWEST, NAVMEDEAST, etc. If you act on your PRD in this timeframe, you’ll be well ahead of the game.
9-12 Months Before Your PRD – This is the traditional detailing window where you contact your Detailer and Specialty Leader to negotiate your next career move. This is when physicians normally submit an extension request as well as explore potential billets for their next set of orders. The one caveat is that the availability of billets is often contingent on the results of the Graduate Medical Education Selection Board or GMESB. Since these results are not finalized until January, people with summer PRDs will find that they may have to wait beyond this time period to find out what billets are available and get orders.
6-8 Months Before Your PRD – This is when the list of billets that are actually available will solidify and most physicians will get orders. If you want to extend at your current command and you haven’t submitted an extension request yet, you should do that ASAP.
1-5 Months Before Your PRD – Many physicians will get into this period without orders. If it is because you were waiting on the results of the GMESB, you are probably fine. If you are in this period for another reason, you should get nervous. The truth is that unanticipated things always happen. Commanding Officers don’t endorse extension requests. Unanticipated openings cause a Detailer and Specialty Leader to have a “hotfill” billet. When things like this happen, a Detailer goes looking for officers close to their PRD to fill the need. If you are in this window without orders, you are low lying fruit for filling these needs. And just so you know, most of these “hotfills” are not in Rota or San Diego.
At Your PRD or Beyond – Physicians let their PRDs “expire” all the time. Sometimes it is because they submit an extension request that never gets approved because it gets lost somewhere in the process. Other times they don’t know when their PRD is. Realistically, there is often no consequence if your PRD expires, although some commands will pick up on this fact and get your attention by threatening to take away your computer access. The biggest threat, though, is the aforementioned “hotfills” that inevitably show up. If your PRD is expired, you are going to rise to the top of the list when the Detailer goes looking for people to fill that need. Have fun wherever that “hotfill” is.
The Bottom Line – Know when your PRD is and manage it according to the above timeline. This will give you the maximum chance of getting what you want and reduce the chance that you are selected for a “hotfill” you don’t want.
Free Military One Source Guide to the Uniformed Services Blended Retirement System
You can get a free guide to the Blended Retirement System from Military One Source here:
MCCareer.org The Book – Chapter 3 – Career Progression and Promotion Board Math
Introduction
When you start your Naval career, the future is largely a mystery. As you progress is your career, things will crystalize, you’ll become wiser, and you’ll think, “It would have been nice to know all of this in the beginning.”
I’m going to try and tell you what you should have known about career progression and promotion board math from the beginning.
Career Progression
This diagram below demonstrates the typical career progression of a Medical Corps officer who has no prior service. Assuming you are not picked early for promotion, you typically promote every six years. You will become a Lieutenant Commander (LCDR) at approximately 6 years, a Commander (CDR) at 12 years, and a Captain (CAPT) at 18 years. I had no prior service, I have never been promoted early, and this is exactly the timing I experienced in my career.

Along the left are the ranges of promotion opportunity for each rank from fiscal year 2013-2020. In each year, the promotion opportunity for LCDR has been 100%. In theory, if all the Lieutenants are suitable for promotion they can all be promoted to LCDR. When it comes to the promotion opportunities for CDR or CAPT, interpreting them is a touch more difficult because we have to talk about promotion board math.
Promotion Board Math
In Fiscal Year 2019 (FY19), people were very excited about a 90% promotion opportunity for the FY19 Staff Corps O6 promotion board. But it was easy to misinterpret this opportunity. It did not mean that 90% of CDRs were selected for CAPT.
Where Does the Promotion Opportunity Come From?
The short answer is from manpower projections. How many physicians are getting out or retiring? What is the current Medical Corps manning level for that rank? What are future needs anticipated to be? What is the size of the promotion zone? The answers to all of these questions determines the promotion opportunity and guide Navy Personnel Command (NPC) and the Bureau of Medicine and Surgery (BUMED) when they are making their decision.
As you can see here, the promotion opportunity varies from year-to-year:
| FY13 | FY14 | FY15 | FY16 | FY17 | FY18 | FY19 | FY20 | |
| LCDR | 100% | 100% | 100% | 100% | 100% | 100% | 100% | Pending |
| CDR | 80% | 80% | 70% | 70% | 65% | 75% | 85% | 77% |
| CAPT | 60% | 60% | 60% | 50% | 70% | 80% | 90% | 81% |
Historical promotion opportunities for FY13-20.
But as you can see here, the percentage who are promoted from the in zone group is substantially lower:
| FY13 | FY14 | FY15 | FY16 | FY17 | FY18 | FY19 | FY20 | |
| LCDR | 97% | 89% | 90% | 93% | 88% | 85% | 87% | Pending |
| CDR | 58% | 66% | 49% | 53% | 44% | 40% | 52% | 53% |
| CAPT | 55% | 43% | 47% | 39% | 34% | 37% | 41% | 51% |
Historical percentage of in-zone candidates selected for promotion for FY13-20.
Promotion Board Zones
There are three “zones” for promotion – below zone, in zone, and above zone. Medical Corps officers are below zone for two years, in zone for one year, and above zone until they are either selected for promotion or get out of the Navy. A few people are usually picked early or below zone, but most people will not get picked until they are in or above zone.
FY19 O6 Promotion Board Math
In FY19, there were 74 CDRs in zone for promotion. To figure out how many officers can be selected for promotion, you have to multiple the zone size by the promotion opportunity. For example, if you take the 90% promotion opportunity everyone was excited about and multiply it by the zone size of 74, you’ll see that they could have promoted 67 CDRs to CAPT during the board:
90% opportunity X 74 people in zone = 66.6 (rounded up to 67) people they can pick for O6
These 67, though, were picked from CDRs who were below zone, in zone, or above zone. Usually, there is a small number picked from below zone, and a much larger number from the in zone and above zone categories. Here were the results:
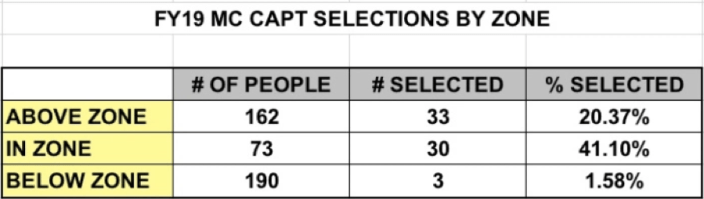
As you can see, the 90% promotion opportunity only led to a 41% selection rate for those who were in zone. The remainder came from the below and above zone CDRs.
The Bottom Line on Career Progression
The typical career progression occurs with a promotion every six years, as detailed in the diagram below. The promotion opportunities listed, though, result in a much lower chance of getting picked when you are in zone because the selections come from those below, in, and above zone.
Post-9/11 GI Bill Education Benefits Transfer Deadline Approaching
Here’s a link to this Navy article:
Post-9/11 GI Bill Education Benefits Transfer Deadline Approaching
NDAA 2020: The Latest on TRICARE, Medical Billet Cuts, and More
Here’s a link to this article from MOAA:
NDAA 2020: The Latest on TRICARE, Medical Billet Cuts, and More
Finance Friday Articles
Here are this week’s articles:
4 Reasons Doctors Don’t Save Enough Money
Don’t Mix Insurance and Investing
GI Bill transfer ban for older troops could be thrown out
Math vs Emotion and Asset Allocation
Roth versus Tax-Deferred: The Critical Concept of Filling the Brackets
Six and a Half Ways to Bridge the Early Retirement Gap to Age 59 and a Half
The Developing Story of Emerging Markets
What is a Safe Withdrawal Rate? A Case Study on The 4% Rule
