Throwback Thursday Classic Post – Tips to Improve Your Concurrent FITREP
An officer e-mailed me and asked for tips on improving his concurrent FITREP, which I thought would make a nice blog post.
A concurrent FITREP is most often received when you are deployed. It is “concurrent” because not only are you getting a FITREP from your deployed command/unit, but you are also getting one from your home/parent command. For example, in 2016 I returned from my last deployment after being gone from September 2015 to June 2016. I received both a periodic FITREP from my parent/home command and a concurrent FITREP from my deployed command.
Tips to improve your concurrent FITREP include:
- Realize that operational commanders often know very little about medical/Navy FITREPs, so you want to do everything you can to make sure that none of these critical FITREP mistakes happen to you.
- Try to get a strong soft breakout where the commander compares you to all officers of the same grade under his/her command either now or during his/her entire career. For example, “In the top 10% of over 200 O4 officers I’ve rated in my entire career.”
- Make sure your most important title/duty is in the box in the upper left of block 29. For example, don’t put “PHYSICIAN” but “OIC” or “SMO”. You can often score some titles that sound very important on a deployment, like “MEU SURGEON” or “GROUP SURGEON”. You don’t want to waste them.
Otherwise, general FITREP advice can be found on my FITREP prep page.
Global Health Engagement Position – Health Affairs Attaché, Vietnam – O5/O6
There is a wonderful global health engagement (GHE) opportunity for an O-5/O-6 physician. We will be filling the Health Affairs Attaché position at the embassy in Hanoi, Vietnam. The desired report date is September 2020.
Applications (CV, Bio, Letter of Intent), with Detailer and Specialty Leader concurrence, should be submitted to CDR Melissa Austin (contact is in the global) NLT COB, Friday, November 22nd.
Here are some additional details:
Know Your Bosses
One of the best ways to prepare for interviews when you are trying to score an important position is to be up to date on issues of focus by senior leadership. Here are a few references of interest.
Secretary of Defense
The SecDef recently put out an unclassified message to his commanders. Here it is:
Message to the Force – Warfighting Readiness
Surgeon General
The new Surgeon General focuses on high reliability principles. If you need a primer on them, here is a good open access article from the Joint Commission:
High-Reliability Health Care: Getting There from Here
Here is also an article he wrote:
Fleet Practices Are Driving Better Health Care
I’m Speaking at the Professional Development Committee Discussion on “The Future of Military Medicine” – NMCP – 14 NOV – 1200-1315
Here’s the info sent out about this panel I’ll be speaking at:
We are one week away from our incredible panel brought to you by the Professional Development Committee on the vital topic, “The Future of Military Medicine”. Our panel has adjusted slightly, but we have just an incredible trio that will be present to discuss the important topics on everyone’s mind as we find our course forward in military medicine. Our very own CO, CAPT Lisa Mulligan, will still be on our panel and will be joined by CAPT Guido Valdes, Deputy Commander of Navy Medicine East, as well as CAPT Joel Schofer, Deputy Chief of the Medical Corps from BUMED. This great, high-powered group will be giving us insight into ways forward from the BUMED, NME, and Command level. We look forward to seeing you all there! Tell your friends. VTC info below.
Conference Name: The Future of Military Medicine
Conference Date: Thursday, November 14, 2019
Conference Location: Auditorium, Building 3, NMC Portsmouth
Here’s a PDF announcement as well:
My Investment Portfolio
I write a lot about personal finance. If you are wondering what I’m doing for my own finances, here’s a detailed look at my own portfolio. I’m not going to give you dollar amounts, but percentages. If you want to know the dollar amounts, they can be expressed in one word. I have…enough:
At a party given by a billionaire on Shelter Island, Kurt Vonnegut informs his pal, Joseph Heller, that their host, a hedge fund manager, had made more money in a single day than Heller had earned from his wildly popular novel Catch-22 over its whole history. Heller responds,“Yes, but I have something he will never have . . . enough.”
Assets
My financial assets from largest to smallest include: (all percentages are rounded to the nearest whole percentage)
- 24% – My taxable mutual funds, which is where I put our retirement savings when I fill our retirement accounts. It is currently invested in:
- 56% – Vanguard Total Stock Market Index Fund Admiral Shares (VTSAX)
- 37% – Vanguard Total International Stock Index Fund Admiral Shares (VTIAX)
- 7% – Vanguard Prime Money Market Fund Investor Shares (VMMXX)
- 21% – My Thrift Savings Plan (TSP) – Currently invested in this proportion:
- 91% – US stocks
- 75% – C Fund
- 25% – S Fund
- 1% – International stocks (I Fund)
- 9% – US bonds split evenly between the G Fund and F Fund
- 91% – US stocks
- 15% – My paid off house.
- 12% – My wife’s TSP, which is invested 100% in US bonds with a 50/50 split of the G and F Funds.
- 12% – My wife’s Roth IRA, which is invested in:
- 53% – Vanguard Total International Stock Index Fund Admiral Shares (VTIAX)
- 47% – Vanguard Total International Bond Index Fund Admiral Shares (VTABX)
- 9% – We have two 529 plans with Vanguard invested in their aggressive age-based portfolio.
- 6% – My Roth IRA, which is 100% invested in the Vanguard Total International Stock Index Fund Admiral Shares (VTIAX).
- 1% – My wife’s individual 401k, which is 100% invested in the Vanguard Total International Stock Index Fund Admiral Shares (VTIAX).
- 1% – My wife has a 401k that is invested in the Fidelity® 500 Index Fund (FXAIX).
Liabilities
None. Aside from credit cards we pay off every month, we’re debt free.
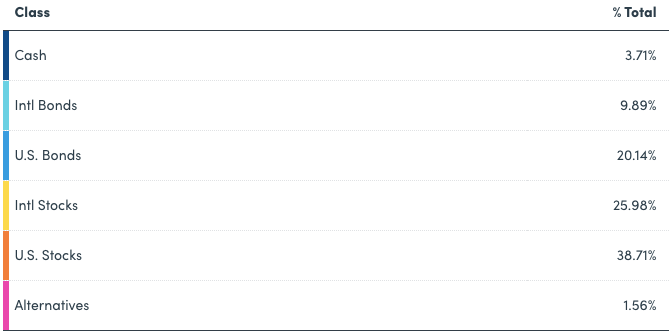
Overall Asset Allocation
Excluding the pension and my house, here’s my overall asset allocation courtesy of our favorite tool that made all of this easy, Personal Capital:
Finance Friday Articles
Here are my favorite articles from this week:
Financial Planning for Early Career Attending Physicians
Following The Stock Market Is Bad For Your Returns
I followed the path to FIRE — and learned that early retirement is the wrong goal
Here are the rest of this week’s articles:
10 Benefits of Keeping Your Credit Score in Good Health
Achieving Work-Life Balance Through Part-Time Work
A Step by Step Guide to Tax Loss Harvesting
Cap Weighted Versus Fundamental Index Funds
How are the 2000 and 2008 retirees doing?
How to Get a Better Deal From a Real Estate Agent
How to Make a Portfolio Rebalancing Spreadsheet
Refinancing Gains in Real Estate
Save first for the kids’ college or for your own retirement?
Top 5 Money Lessons for Physicians
Throwback Thursday Classic Post – You Didn’t Make CDR. Now What?
I receive questions all the time about what happens when you are passed over for promotion and are now “above-zone”. If you find yourself in this position, here is what you need to do:
- Realize that it is not the end of the world. Based on the FY20 CDR promotion board statistics, 47% of in zone officers were passed over, but a large number of the officers selected were from the above zone group.
- If you do nothing, you will continue to get looked at by promotion boards until you retire, resign, or are forced out of the Navy. There is no limit on the number of chances you get to promote and your record will be evaluated for promotion every year. That said…
- You need to try to promote. At a minimum, you should consider sending a letter to the promotion board. What do you say in this letter? First, briefly state that you want to be promoted and to continue your career in the Navy. Second, explain what a promotion would allow you to do that you can’t do at your current rank. Answer the question, “Why should they promote you?” For example, if you want to be a Department Head at a large military treatment facility (MTF) or a Residency Director (or whatever you want to do), tell them that you need to be promoted to CDR to be competitive for these jobs. The Navy wants to promote leaders. Make it clear to them that you are a motivated future leader.
- Try and get letters of support to attach to your letter. These letters should be from the most senior officers who can personally attest to your value to the Navy. In other words, it is probably better to get a letter from an O6 who knows you well than a 3 star who doesn’t. If you are not sure who to ask for letters, ask those more senior to you or your Detailer for advice. Your Specialty Leader is always someone to consider if he/she knows you well and can speak to your contributions to the specialty and Navy.
- Have your record reviewed by your Detailer, Specialty Leader, other trusted senior advisor, or by me. Because of promotion board confidentiality, you will never know the reason(s) you did not promote, but most of the time experienced reviewers can come up with an educated guess. They’ll often find things that you were not even aware of, like potentially adverse fitreps, or information missing from your record. My promo prep document will help you as well.
- Do everything you can to get “early promote” or “EP” fitreps. This is largely accomplished by continually striving for positions of increased leadership. You need to get a job that has historically led to a promotion. As a LCDR who got passed over for CDR, try to get one of these jobs and excel at it (this list is not exhaustive and these positions are not the only path to CDR, but they are a good start):
- Medical Executive Committee (MEC) member
- SMO on an amphibious platform
- Regimental Surgeon
- Member of a hospital committee or chair of a smaller committee
- Department Head in a small MTF
- Medical Director/Senior Medical Officer in a medium/large MTF
- Detailer
- Meet with your chain-of-command. After you’ve been passed over is not the time to be passive. You need to sit down with your leadership and get an honest assessment from them of how you’re doing and what they would recommend continuing to advance your career. You may not like what you hear, but it is better to find out early if they don’t think you’re doing a good job or that you are unlikely to break out on your fitreps. That way you can try and put yourself in a better situation by changing commands.
In addition to the above list of things you should do, there are a few things you should not do:
- Do not lie in your letter to the board. In other words, don’t tell them you want to do Executive Medicine if you don’t really want to. Your record reads like a book, and if it tells a story that is contrary to what your letter says, this is unlikely to help you and may hurt you.
- Do not send long correspondence. Promotion boards have to read everything sent to them, and a long letter may not be appreciated. Keep it brief and to the point.
- Do not ask your current CO to write you a letter to the board if they’ve done an observed fitrep on you. His or her opinion about you should be reflected on that fitrep, so they don’t need to write you a letter. If they’ve never given you an observed fitrep or there is some new information not reflected on prior fitreps, they could either write you a letter or give you a special fitrep. Ultimately it is up to them whether they do either of these or none.
- Do not discuss anything adverse unless you want the board to notice and discuss it. This issue comes up frequently and people will ask me for advice, but ultimately it is up to the individual officer. The one thing I can guarantee is that if you send a letter to the board and discuss something adverse, they will notice it because they will read your letter! If you think there is a chance the adverse matter will get overlooked, it is probably better not to mention it and keep your fingers crossed.
Those are my tips for those who find themselves above zone. Most importantly, if you want to promote, NEVER STOP TRYING. You can usually stay in as a LCDR for 20 years, and I personally know of people who got promoted their 4th look and have heard of people who succeeded on their 9th try!
Help Us With HPSP Recruiting
The Corps Chief’s Office is looking to identify Medical Officers who have a connection to any of the following undergraduate schools in order to facilitate high-yield Health Professions Scholarship Program (HPSP) recruiting. We are exploring options for funded TAD, but no promises can be made at this time. If you could please forward to your communities, asking anyone who would be willing to meet with pre-medical societies and recruit for HPSP to email CDR Brett Chamberlin at brett.m.chamberlin.mil < at > mail.mil, we will be compiling a master list of potential MC Officers for this initiative.
Please include Name, Rank, Current Duty Station, willingness to travel unfunded (with permissive TAD)
- University of Michigan
- Michigan State University
- University of Texas
- Texas A&M University
- The Ohio State University
- University of Georgia
- Emory
- University of Wisconsin
- Rutgers University
- Brigham Young University
- University of South Florida
- Washington University in St. Louis
- University of Arizona
- Arizona State University
Top Schools Proximal to NMRTCs:
- University of Florida
- UC San Diego
- UNC Chapel Hill
- University of Washington
- University of Virginia, Charlottesville
- Johns Hopkins
- Florida State University
- UC Irvine
- University of Maryland, College Park
- Duke
